Malnutrition that occurs when the body does not receive enough food.
Malnutrition results in progressive weight loss. It is common in older people, especially those with Alzheimer’s disease. Depending on whether the person is at home (10%), in an institution (30%), or in the hospital (70%), its prevalence differs.
A person suffering from undernutrition may be deficient in vitamins, minerals, and other essential substances that the body needs to function.
Malnutrition can lead to:
short-term and long-term health problems
slow recovery from injury and illness
a higher risk of infection
difficulty concentrating at work or school
Certain deficiencies can trigger specific health problems.
For example a lack of vitamin C can lead to scurvy. Although rare in developed countries, it can develop if a person does not eat a varied diet with plenty of fresh fruits and vegetables.
Older people who drink heavily and people with certain mental health conditions may be particularly at risk. Undernutrition is particularly common in people over 60 years of age. Weight loss in this category approximately doubles the risk of dying.
Malnutrition symptoms
Some signs and symptoms of malnutrition include:
a lack of appetite or interest in food or drink
tiredness and irritability
an inability to concentrate
always be cold
the Depression
loss of fat, muscle mass, and body tissue
a higher risk of getting sick and taking longer to heal
longer healing time
a higher risk of complications after surgery
Eventually, a person may also experience difficulty breathing and heart failure.
The causes
Undernutrition can occur for a variety of reasons.
Low food intake
Some people are undernourished because there is not enough food available or because they have difficulty eating or absorbing vitamins and minerals.
This can happen as a result of:
cancer
liver disease
disorders that cause nausea or make it difficult to eat or swallow
taking medications that make it difficult to eat – for example due to nausea
Mental health problems
Undernutrition or malnutrition can affect people with:
depression
dementia
schizophrenia
anorexia nervosa
Social and mobility issues
Factors that can affect a person’s eating habits and potentially lead to undernutrition include:
being unable to leave the house or go to a store to buy food
find it physically difficult to prepare meals
living alone, which can affect a person’s motivation to cook and eat
have limited cooking skills
not having enough money to buy food
Digestive disorders
If the body does not absorb nutrients efficiently, even a healthy diet may not prevent undernutrition.
Here are examples of digestive and gastric conditions that can cause it:
Crohn’s disease
celiac disease
persistent diarrhea, vomiting, or both
Alcohol use disorder
Consuming a lot of alcohol can lead to gastritis or long-term damage to the pancreas. This can make it difficult to digest food, absorb vitamins, and produce hormones that regulate metabolism.
Alcohol also contains calories, so a person may not feel hungry after drinking. She may therefore not be eating enough healthy foods to provide the body with essential nutrients.
Malnutrition and Alzheimer’s disease
Between 20 and 45% of patients with dementia are undernourished and lose weight in the year following the onset of their disease, according to the report entitled “Nutrition and dementia”, from Alzheimer’s Disease International (ADI, February 11, 2014) .
Energy malnutrition results from an imbalance between the body’s intake and needs, leading to tissue loss (including muscle), which has deleterious functional consequences.
In addition, 10% of elderly people at home suffer from undernutrition, and this percentage rises to 30% when they are placed in a retirement home. Finally, this is the case for 70% of hospitalized elderly people.
In people with dementia, malnutrition can be the cause of falls or worsening cognitive impairment.
The Association even suggests that undernutrition is a triggering factor for certain forms of dementia.
The report says that certain measures can be taken to improve the nutrition of patients with dementia. These measures include setting nutritional standards, better monitoring the weight of patients, looking at diet and eating habits regularly, and training the family and professional environment.
This malnutrition may be due to cognitive deficits and loss of autonomy or to an increase in energy expenditure (wandering, hyperactivity).
Protein-energy malnutrition
A disorder characterized by a negative balance of protein and energy, leading to loss of weight and muscle mass. Malnutrition can have several causes:
– Diet that does not meet nutritional needs in protein and energy.
– Poor intestinal absorption.
– Increased nutritional needs following an acute or chronic illness.
– Abnormally large losses caused for example by a nephrotic syndrome or a wound.
It is often observed in elderly people of fragile constitution, living or not in an institution or hospitalized.
Protein-energy malnutrition is retained when, among other things, the elderly person:
– involuntarily loses more than 5 kg.
– Has a body mass index of less than 21 kg/m2.
– Has a Mini Nutritional Assessment test result of less than 17.
The consequences of undernutrition
The consequences are as follows:
weightloss;
appearance of bedsores;
falls and fractures;
lowered immune system;
bacterial infections (urinary, bronchopulmonary);
hospitalization.
Evaluation
It requires:
a weight curve;
an assessment scale such as the Mini Nutritional Assessment or the Mini Nutritional Assessment Short Form.
Some patients affected by advanced Parkinson’s disease may suffer from cognitive disorders and more generally from a specific form of dementia.
There are other neurodegenerative diseases that can cause both motor and cognitive impairment: dementia with Lewy bodies, progressive supranuclear palsy, multiple system atrophy and corticobasal degeneration.
Lewy body dementia
It is characterized by the existence of lesions called Lewy bodies.
Progressive supranuclear palsy
This disease, also called Steele-Richardson-Olszewski disease, usually begins after the age of 40. Its prevalence is 1.4/100,000 versus 100 to 170/100,000. It is characterized by a decline in ocular motor skills (especially vertical gaze), postural instability with frequent falls and akinesia.
There are differences with Parkinson’s disease: – Significant axial stiffness in the neck. – Dysarthria (speech disorder linked to neurological impairment). – Dysphagia (discomfort in swallowing). – Minor tremor. – Significant postural problems. – Motor disorders do not improve after treatment with L-dopa or a dopaminergic agonist. – Cognitive disorders of the frontal type appear during the evolution.
These disorders are caused by damage to the basal ganglia and brainstem, with the presence of neurofibrillary tangles including the abnormal form of tau protein.
Multiple system (or multiple system) atrophy
It is a set of neurodegenerative diseases including: – degeneration of the nigrostriatal pathway, with an extrapyramidal syndrome characterized by rigidity and akinesia. The damaged cerebral structures are the substantia nigra and striatum and involved in motricity are affected. – Shy-Drager syndrome, with dysautonomia (dysfunction of the autonomic nervous system. – Olivo-pontocerebellar atrophy with cerebellar syndrome. The cerebral structures called pons nuclei and the cerebellum are affected.
The occurrence of cognitive disorders can be observed in advanced forms. Levodopa (reference treatment for Parkinson’s disease) only partially responds to the extrapyramidal syndrome.
Corticobasal degeneration
It is caused by damage to the frontal and temporal cortex, as well as damage to the basal ganglia. The neurons are said to be ballooned (ie swollen) and surrounded by glial cells which proliferate (we speak of a phenomenon of gliosis).
Clinically, the disease is characterized by apraxia and extrapyramidal syndrome.
Apraxia often begins in one part of the body, causing the inability to perform elaborate movement, despite good understanding and normal muscle strength.
The extrapyramidal syndrome is asymmetrical, even unilateral and is limited to akinesia and rigidity. However, there may be postural tremor, dystonic disorders usually beginning in the upper limb, myoclonus (rapid, involuntary, low-amplitude muscle contraction) and apraxic disorders.
The cognitive impairment appears during the evolution with behavioral disorders and signs of frontal dementia. Treatment with levodopa (or L-Dopa) has no effect. Myoclonus can be treated with clonazepam (a benzodiazepine).
The signs of dementia – a syndrome whose term appeared at the beginning of the 19th century – are characterized by different disorders:
memory ( these are early disorders);
other higher functions: orientation, attention, judgment, reasoning;
phasic (difficulties reading, speaking, reading, writing or repeating a sentence;
praxis (inability to perform motor tasks despite intact motor skills);
gnostic (lack of recognition of familiar objects despite intact sensory functions);
executive functions (loss of sense of abstraction, planning, initiation and organization of tasks).
These cognitive disorders are generally accompanied by psychological and behavioral signs and symptoms (apathy, depression, agitation, aggressiveness, irritability, wandering, insomnia, delusions, etc.) that can affect activities of daily living.
The symptoms of dementia have two main characteristics:
Symptoms appear in adulthood (mental retardation is not one of them).
The symptoms are in most cases progressive and irreversible (confusions and depressive states of the elderly are not included).
Signs of cognitive impairment in dementia
Cognitive disorders
Examples
Inability to learn recent information and events
• The subject involuntarily makes the same purchase several times during the day. • The subject repeats the same question.
Loss of orientation (especially temporal)
• The subject wanders for several hours in his neighborhood and no longer knows how to get home. • He cannot name today’s date.
Difficulties performing an abstract task
• The subject becomes distraught in front of a tax form because he has difficulty performing simple calculations or recognizing numbers. • Subject cannot plan a subway trip requiring one or more connections.
Difficulties finding words
• The subject compensates for the omission of words by using other words such as “trick, thing, contraption”. • The subject uses phonemic verbal paraphasias (says lion instead of violin). • The subject uses sentences that are difficult to understand.
Misplaced objects
Subject puts dirty clothes in a closet and does not remember where they have been stored.
Difficulties understanding symbols
Subject no longer recognizes a road sign.
Forgetting old facts
The subject forgets the name of a famous person, a birthday.
Poor or impaired judgment
The subject dresses warmly on a very hot summer day, or goes shopping in a dressing gown
Difficulty performing familiar tasks
• The subject has difficulty using household appliances. • Subject has difficulty preparing a meal. He forgets to serve it or to have prepared it.
Is memory the only one affected in dementia?
No, these cognitive disorders are accompanied by changes in mood, behavior and a loss of initiative.
Here are some signs of behavioral dementia:
Asocial behavior For example: the subject is apathetic, sits idle, remains indifferent, has little interest in others, cuts off all contact with friends, abandons leisure activities.
Sadness
emotional lability
Irascibility or even verbal and physical aggression
Suspicion
Fearful behaviors
Social disinhibition
Appearance of excessive familiarity
Noisy behaviors
Euphoria, boundless energy
Episodes of depression and anxiety (the subject becomes aware of his cognitive disorders)
Insomnia
Paranoia
Hallucinations visual, auditory (rare)
Slower movement speed
Signs of dementia that affect daily life
Difficulty driving
Wandering
Forgetting to serve a dish cooked in the oven
Negligence (housework, toilets, etc.) or carelessness
Difficulties managing expenses
Professional errors
Difficulties making purchases
Why does the subject or his entourage ask to be consulted?
At an early stage, it is usually for memory disorders (appearing gradually) that the subject or most often a member of his or her entourage asks to be consulted (in 75% of cases, memory disorders presage dementia of the Alzheimer type ). Studies have shown that, in 30% to 50% of cases, the cognitive deficit is ignored by the person concerned.
Rarer are dementias of the Alzheimer type beginning with behavioral disorders. In the case of disorders that are already visible and seem to be getting worse, the request comes from the family and medical environment. It is then a question of behavioral disorders whose appearance or aggravation provoke a crisis in the family care.
What are the different stages during the consultation?
Whether or not the doctor makes a diagnosis following:
An anamnesis which is a series of information provided by the subject (eg medical history) and confirmed if necessary by those around him. The doctor assesses the subject’s functional abilities (eg ability to carry out physical activities of daily living).
Basic exams.
A clinical physical examination which assesses in particular the mental faculties of the patient, in particular with the mini-mental state examination, which is the test used.
If a diagnosis of dementia is made, the next step is to determine the underlying cause.
The causes may be reversible (depression, delirium, ‘toxic’ side effects of medication, infections, etc.) or irreversible (Alzheimer’s type dementia, vascular dementia, frontotemporal dementia, Lewy body dementia, dementia associated with Parkinson’s disease, etc.).
Alzheimer’s disease is the most common cause of dementia (about 60% of dementia cases).
In summary
Cognitive disorders + emotional and behavioral disorders + disturbances in daily activities:
=> suspected dementia.
=> medical visit.
=> if dementia, search for the reversible or irreversible cause.
Vascular dementia is recognized as multiple infarct dementia resulting from successive strokes.
It was described at the end of the 19th century by doctors Binswanger and Alzheimer.
Vascular dementia includes heterogeneous categories of vascular diseases, excluding those caused by asphyxia, respiratory failure or carbon monoxide poisoning.
It varies depending on the location and type of lesions associated with it. In nearly 70% of cases, these lesions affect the small vessels and the white matter in the regions below the cortex (eg the amygdala).
Most studies indicate that vascular dementia is the second leading cause of dementia after Alzheimer’s disease, accounting for between 10 out of 20% of cases.
The prevalence of the disease varies from 1.2 to 4.2% in people aged 65 and over.
These figures should be taken with caution because unlike Alzheimer’s disease, there is no consensual definition and valid diagnostic criteria for vascular dementia. In addition, brain imaging is generally not performed in population studies.
The differential diagnosis between Alzheimer’s disease and vascular dementia is sometimes difficult because, on the one hand, the latter is not always associated with a vascular event and, on the other hand, its clinical evolution is gradual as in Alzheimer’s disease.
The causes of vascular dementia
There are several forms of lesions that cause the different forms of vascular dementia. These diseases are divided according to the regions of the brain affected, their frequency, and the size of the arteries and vessels affected. There is no official classification of vascular dementias, but they can be classified as follows, inspired by the classification proposed by the clinician Roman.
Dementia caused by multiple and extensive cerebral infarctions (or strokes), affecting cortical and subcortical regions that play a role in cognitive functions. These infarctions are often accompanied by mini-lesions damaging the white matter. Although this form reflects the classic view of vascular dementia, it is not the most common.
Clinical signs: focal neurological signs, cognitive disorders such as aphasia, apraxia, agnosia.
Its evolutionary course describes either a sudden onset and a stepwise worsening (one-third of cases), or an insidious onset and gradual evolution (one-third of cases).
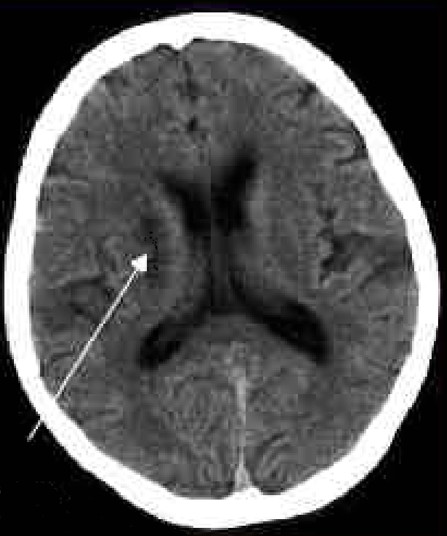
2. Dementia caused by single lacuna-sized brain infarctions affecting a specific cortical and subcortical region that plays an important functional role. Cortical regions affected are the medial temporal lobe, angular and cingulate gyrus, while subcortical regions affected are the thalamus, caudate nucleus, internal capsule and anterior cerebral artery. These infarcts generally affect both hemispheres.
3. Dementia caused by damage to small vessels (also called subcortical ischemic vascular dementia). These small vessels are either obstructed by atherosclerosis leading to the formation of several gaps, or narrowed (phenomenon of stenosis) leading to partial infarctions of the white matter . This dementia affects subcortical regions (as seen in Binswanger’s disease, rare CADASIL, multiple lacunae), or cortical and subcortical regions (arteriolosclerotic and hypertensive angiopathy, amyloid angiopathy). This form of dementia presents with mini-lesions or multiple white matter lacunae, located particularly in the frontal regions.
Clinical signs: psychomotor and balance disorders, urinary incontinence, cognitive disorders (executive functions and to a lesser extent memory) and behavior (mood). Balance disorders worsen as the disease progresses. Patients become increasingly apathetic, exhibit rapid and significant changes in mood (emotional lability), loss of attention, perseverations (stereotypical behavior of repeating the same word, performing the same movement, in response to various questions or tasks requested).
4. Dementia caused by hypoperfusion:
• Diffuse anoxic encephalopathy (anoxic: decrease in the amount of oxygen). • Incomplete white matter infarction.
5. Hemorrhagic dementia, caused by subdural hematoma (hematoma of the meningeal spaces, between the arachnoid and the dura mater), subarachnoid hemorrhage, or venous thrombosis. MRI has identified chronic hemorrhagic lesions characterized by the presence of hemosiderin deposits (iron deposits impregnating the tissues).
Lacunae affecting the thalamus (arrow), cerebral region located below the motor regions of the basal ganglia.
Diagnostic criteria
There are at least eight diagnostic criteria for vascular dementia, reflecting the lack of consensus among the medical community. The main ones are: Hachinski ischemic score, DSM-IV, NINDS-AIREN criteria, ICD 10, ADDTC criteria (State of California Alzheimer’s Disease Diagnostic and Treatment Center).
NINCDS–AIREN Criteria
These criteria divide the patient into three stages: probable, possible and definite vascular dementia. The three criteria for probable vascular dementia:
Presence of dementia characterized by impairment of episodic memory and at least two other cognitive domains: orientation, attention, language, visual and spatial abilities, executive functions, motor control and praxis. They are significant enough to interfere with activities of daily living. Exclusion criteria: impaired consciousness, confusion, psychotic symptoms, severe aphasia, major sensorimotor disorder preventing neuropsychological assessment, other brain diseases (such as Alzheimer’s disease).
Presence of cerebrovascular disease defined by focal neurological signs (hemiparesis, central facial paralysis, Babinski’s sign, sensory deficit, hemianopsia, dysarthria on neurological examination, and the presence of cerebrovascular disease demonstrated by brain imaging.
A relationship between dementia and cerebrovascular disease manifested by the presence of at least one of the following three points:
onset of dementia within 3 months of stroke
sudden deterioration of cognitive functions;
a fluctuating or stair-stepping course of cognitive impairment;
Elements supporting the diagnosis of vascular dementia:
presence of an early gait disorder (walking with small steps);
a history of instability or frequent unprovoked falls;
urinary disorders unexplained by a urological condition;
pseudobulbar palsy;
personality or mood changes, abulia, depression, emotional lability, psychomotor retardation and executive function abnormalities.
The diagnosis of vascular dementia is questioned if the progressive deterioration of cognitive functions is not accompanied by vascular lesions (validated by scanner or MRI) or neurological signs.
The criteria for possible vascular dementia are:
presence of dementia and neurological signs when no neuroimaging study is available or;
no clear temporal relationship between dementia and stroke or;
insidious onset and variable fluctuating course of cognitive deficits.
The criteria for definite vascular dementia are:
a clinical history of probable vascular dementia;
anatomical evidence of cerebrovascular disease (e.g. after autopsy);
absence of neurofibrillary tangles and abnormally high amyloid plaques for age;
the absence of other clinical or pathological signs capable of causing dementia.
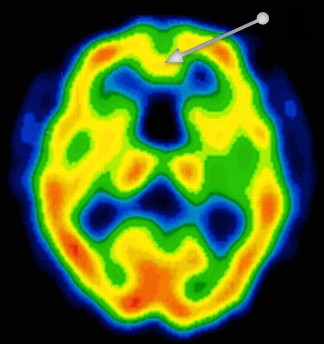
Magnetic resonance imaging of a brain of a person with vascular dementia. In the region of the frontal lobe (arrow), a decrease in cerebral blood flow significant of a severe lesion is observed. This decrease is characterized by a yellow color, while the red color reflects a normal flow. The lesion is characteristic of neuronal death leading to a decrease in oxygen consumption by the neurons.
Brain imaging techniques
The different cerebral imaging techniques make it possible to determine the presence of significant anomalies responsible for the different types of vascular dementia. They complete the diagnostic criteria.
Forms of brain imaging are:
Magnetic resonance imaging, the most widely used method to assess cerebrovascular pathology.
Functional magnetic resonance imaging. It assesses how the functions of different brain regions are reorganized following vascular dementia.
Positron emission tomography (PET) imaging. It is a technique that measures the metabolic activity of brain regions by injecting the radioactive tracer called 18-fluorodeoxy-D-glucose. In vascular dementia, decreased metabolism is seen in the association cortex (as in Alzheimer’s disease), primary cortices, basal ganglia, thalamus, and cerebellum.
Single photon emission tomography (SPECT). Unlike PET, SPECT only detects a single photon (while PET detects two), which decreases the spatial resolution of the images. However, it is a much more accessible method, because on the one hand the radiotracers are more available (they do not require emitting positrons) and on the other hand the imaging system is simpler.
Despite the usefulness of these techniques, functional neuroimaging cannot distinguish the lesions associated with Alzheimer’s disease from those observed in vascular dementia.
Blood tests
Doctors may need to order lab tests to check for health indicators that aren’t apparent in a person’s recent medical history. This may include tests to check their cholesterol or blood sugar levels.
They may also order additional tests to help rule out other issues that may be causing similar symptoms, such as vitamin deficiencies, anemia, and thyroid disorders.
The signs and symptoms
Cognitive functions
Vascular dementia is characterized by:
early impairment of executive functions (planning, abstract thoughts),
attention deficit, decreased verbal fluency (semantic memory disorder) and
deterioration of visual-spatial functions.
These 3 types of cognitive disorders are more marked than in Alzheimer’s disease.
On the other hand, episodic memory is less affected in vascular dementia than in Alzheimer’s disease.
There is a correlation between the location of brain damage and the type of cognitive impairment patients suffer from.
With regard to vascular accidents of small vessels, characterized by lesional damage limited to the subcortical regions, cognitive deficits are quite frequently limited to impaired executive functions (flexibility, inhibition, working memory). Memory damage, characterized by a deficit in retrieving a memory, makes it possible to differentiate these disorders from those observed in Alzheimer’s disease.
With regard to vascular accidents of the large vessels (lesional damage affecting both the cortical and subcortical regions), establishing a differential diagnosis proves to be much more difficult. In general, episodic memory (measured by the word recall test) is better preserved in vascular dementia than in Alzheimer’s disease. Degradation of working memory (characterized for example by the ability to repeat a series of numbers) is also very common in this type of lesion.
Some clinicians suggest removing the notion of memory decline as a diagnostic criterion.
Functional autonomy
Functional decline in basic activities of daily living appears to be identical in vascular dementia and Alzheimer’s disease, whereas decline in instrumental activities of daily living (eg managing money) appears slower in vascular dementia.
Behaviour
Behavioral disorders are generally similar to those observed in Alzheimer’s disease. Depressive symptoms, emotional behavioral disturbances, and apathy appear to be more common in vascular dementia than in Alzheimer’s disease.
Risk factors for vascular dementia
Risk factors for vascular dementia can include smoking, obesity, and high blood pressure.
The risk of vascular dementia tends to increase as a person ages. The National Heart, Lung, and Blood Institute states that the disease affects nearly a third of people over the age of 70.
Additionally, a number of other factors and conditions can increase the risk of damaged blood vessels and vascular dementia, including:
smoking
obesity
abnormal heart rhythms
high cholesterol
high blood pressure
atherosclerosis
diabetes
a history of heart attack or stroke
Evaluation of vascular dementia
Cognitive functions
The Alzheimer’s Disease Assessment Scale (ADAS-cog), a scale used in Alzheimer’s disease, explores numerous functions (memory, comprehension, temporal-spatial orientation and spontaneous language) altered in vascular dementia. The Trail Making B (tracing test) or the EXIT-25 are used in addition to assess executive functions.
Functional autonomy
Functional decline in basic activities of daily living appears to be identical in vascular dementia and Alzheimer’s disease, whereas decline in instrumental activities of daily living appears to be slower in vascular dementia.
The Disability Assessment in Dementia Scale (DAD) and the Interview for Deterioration in Daily Living Activities in Dementia (IDDD) are functional scales taking into account the consequences of executive function disorders in dementia. These scales make it possible to determine whether the functional incapacity originates from a cognitive deficit (for example difficulty handling money) or a motor deficit (difficulty walking).
Behaviour
The Neuropsychiatric Inventory is, together with the Behave-AD, an appropriate rating scale.
Vascular dementia and Alzheimer’s disease: the differences
There are many differences between vascular dementia and Alzheimer’s disease: prevalence, causes, clinical signs.
Prevalence
Alzheimer ‘s disease is by far the most common type of dementia. It accounts for about two-thirds of dementia cases.
It is estimated that vascular dementia accounts for 10% to 20% of dementia cases.
About 50% of older people with dementia (especially Alzheimer’s type) show signs of vascular dementia. We then speak of mixed dementia if the vascular dementia is associated with dementia of the Alzheimer type.
The causes
Vascular dementia is often caused by a specific acute event, such as a stroke or a transient ischemic attack in which blood flow to the brain has been interrupted. It can also develop more gradually over time as a result of slow blood flow.
The causes of Alzheimer’s disease are not understood, although it is known to be characterized by a buildup of proteins in the brain called amyloid and tau. There seem to be many components, such as genetics, lifestyle, and other environmental factors.
Diagnostic criteria
Alzheimer’s disease
Vascular dementia
1. Presence of dementia 2. Onset between 40 and 90 years of age 3. Deficits in at least 2 cognitive domains 4. Progression of deficits lasting longer than 6 months 5. Unimpaired state of consciousness 6. No other diagnosis made .
1. Presence of dementia 2a. Focal neurological signs 2b. Vascular lesions observed by cerebral imaging 3. Association of 1 and 2 with either: – the existence in the previous 3 months of a cerebrovascular accident or; – sudden cognitive deterioration.
Clinical profiles
The differences between vascular dementia and Alzheimer’s disease also concern the clinical signs.
In the case of vascular dementia: cognitive abilities often seem to decrease sharply in relation to an event such as a stroke or transient ischemic attack (TIA), then remain stable for a period of time.
In the case of Alzheimer’s disease, cognitive functions gradually decline over time. There are usually no sudden, large changes from one day to the next.
Alzheimer’s disease
Vascular dementia
Attention intact
Attention intact
Impaired short and long term memory, amnesia
Failing short-term memory , difficulty in retrieving information. Long-term memory is normally intact.
Poor speech
Poor language
Impaired visual and spatial function
Impaired visual and spatial function
Absence of localized lesions
Presence of localized lesions
Personality change with predominant apathy
Psychosis and agitation in the late phase of the disease
Motor disorders appear only in the severe stage of the disease
Neurological disturbances may be subtle (eg, decreased arm swing when patient is asked to walk on heels or tiptoes). Other neurological disorders are dysarthria, parkinsonism, incontinence and a change in gait.
Poor speech, loss of meaning of words
Poor language, loss of meaning of words
Impaired executive functions
Faulty executive functions
Predominant apathy followed by a psychotic state and agitation in the late phase of the disease
Predominant apathy rarely accompanied by a psychotic state
Absence of localized lesions
Presence of localized lesions
Treatments
There is currently no cure for vascular dementia because there is no way to reverse brain damage. However, it may be possible to slow or sometimes stop the progression of the disease by controlling certain risk factors, for example.
Antihypertensives
Antihypertensives are recommended in hypertensive individuals to reduce the risk of cardiovascular disease. However, there is no consensus regarding the effectiveness of these drugs in reducing the risk of dementia. A study published in 2013 reports this fact, but points out that calcium channel blockers (e.g. lercanidipine, nitrendipine) seem more effective. Some clinicians point out that lowering blood pressure can have deleterious effects in people with cerebrovascular disease. Further studies are needed to determine optimal blood pressure in individuals at risk for vascular dementia.
Antidiabetics
Blood sugar management is recommended in the prevention of diabetes-related complications. The studies that have analyzed the association between diabetes and dementia are not of good enough quality to draw a conclusion.
Statins
Taking statices reduces the risk of dementia in people with high cholesterol. However, if we look at the different forms of dementia, there is no association between taking statins and the risk of vascular dementia.
Antiplatelets
To date, there is no evidence that regular aspirin consumption reduces the risk of developing vascular dementia and slows its progression.
The results of a phase III clinical trial have shown that the combination of anticoagulant drugs (clopidogrel (Plavix) and aspirin) – decreases the risk of recurrence by about a third in patients who have suffered a transient ischemic attack . This decrease is compared to the group of patients who received only aspirin. 8.2% of patients taking both drugs relapsed within three months compared to 11.7% in those taking only aspirin (Source: Clopidogrel with Aspirin in Acute Minor Stroke or Transient Ischemic Attack. New England Journal of Medicine, 2013).
Vitamin B
B vitamins are prescribed to lower blood homocysteine, new highs of which are a cardiovascular risk factor. Several studies have shown the effectiveness of a combination of vitamins B2, B6 and B12 in elderly people suffering from vascular diseases. However, although homocysteine levels were reduced, this treatment was not accompanied by an improvement in cognition.
Lifestyle
It is recognized that the adoption of a healthier lifestyle (stopping smoking, moderate alcohol consumption, physical activity and healthy eating) is associated with better cognitive performance towards old age. Observational studies indicate that intellectual activity (eg bridge) is associated with a reduced risk of mixed and vascular dementia, as well as cognitive impairment of vascular origin.
In addition, such a reduction in risk is observed in those who practice physical activity frequently, compared to inactive people.
Acetylcholinesterase inhibitors
Lack of acetylcholine – the memory neurotransmitter – in the brain is not only seen in Alzheimer’s disease, but also in vascular dementia.
The three acetylcholinesterase inhibitors, aimed at increasing the level of this neurotransmitter in the brain, are also prescribed in the treatment of vascular dementia.
Calcium channel blockers
A meta-analysis concludes that nimodipine (90 mg/day) improves some aspects of cognition, but has no positive effects on activities of daily living. Clinical studies over longer periods (one to two years) are needed to confirm these results. No beneficial effects have been reported with nicardipine and cyclandelate.
Clinical case
A 75-year-old patient is undergoing abdominal surgery. Following this operation, she was again hospitalized for incoherent speech and occasional hallucinations. He was diagnosed with postoperative confusion, cognitive impairment (his mini-mental state exam score was 16/30), and mood disorders.
The doctor prescribed him an antidepressant and an antipsychotic. She then returned to her nursing home. A year later, the patient presented with Parkinsonian-like symptoms (tremor, rigidity) which, together with a cognitive deficit, suggested dementia with Lewy bodies. The doctor prescribed Aricept (a drug used in the treatment of Alzheimer’s disease) and piripedil.
Four years later, the patient entered a long-term care center because she frequently fell due to severe limb rigidity and psychomotor retardation. The treatment with the neuroleptic (known to cause motor disorders) is then stopped. His cognitive performance stabilized with an MMSE score identical to that obtained four years previously. However, she suffers from temporal disorientation, moderate executive function disorders, difficulty memorizing information and retrieving it.
The medical staff suggested the existence of subcortical frontal dementia. However, the neuroimaging examination (magnetic resonance imaging) reveals the presence of ischemic-type vascular lesions as well as diffuse leucoaraiosis.
Diagnosis of this clinical case: the patient probably suffers from vascular dementia.
1 Piripédil (trade name: Trivastal®, France): medicinal product used in particular in the adjunctive treatment of chronic pathological cognitive and neurosensory deficit in the elderly (excluding Alzheimer’s disease and other dementias).
Frontal subcortical dementia is a form of dementia characterized by attention disorders, slowed cognitive performance, severe dysexecutive syndrome, decreased verbal fluency and elaborate language, constructive apraxia (loss of ability to executing gestures or using objects, without any paralysis).
Practical case of frontal subcortical dementia
Mr. A. was diagnosed with Alzheimer’s disease upon entering a long-term care facility with a Mini-Mental State Examination (MMSE) score of 16/30.
His GMP is 850, which means he is very addictive. GMP stands for Weighted Average GIR. It corresponds to the average level of dependency of residents of a long-term care facility in France. The higher the GMP, the greater the level of resident dependency. Generally speaking, a GMP greater than 300 corresponds to a medical establishment. An establishment with a GMP greater than 700 corresponds to a geriatric hospital.
Long-term care takes care of elderly patients, the vast majority of whom have memory problems which are often the reason for their placement.
The medical staff suspected that the diagnosis made before the patient arrived at the facility was incorrect because his cognitive state was not deteriorating.
He continued to memorize names well, to orient himself well in space and to remember past events concerning him (autobiographical memory). In addition, he obtained a score of 20/30 on the MMSE five years after entering the establishment, an increase of 4 points.
A neuropsychometric assessment and a neuroimaging examination (magnetic resonance imaging) indicate that the pathology from which Mr. A. suffers is not characteristic of Alzheimer’s disease.
Neuropsychometric assessment
The patient’s cognitive performance declines only slightly, with mild time orientation disorder , episodic memory encoding and retrieval disorder, dysexecutive syndrome, mild selective attention deficit, mild apraxia ideomotor, as well as difficulties in performing mental calculations.
Neuroimaging examination: the diagnosis of subcortical frontal dementia is made
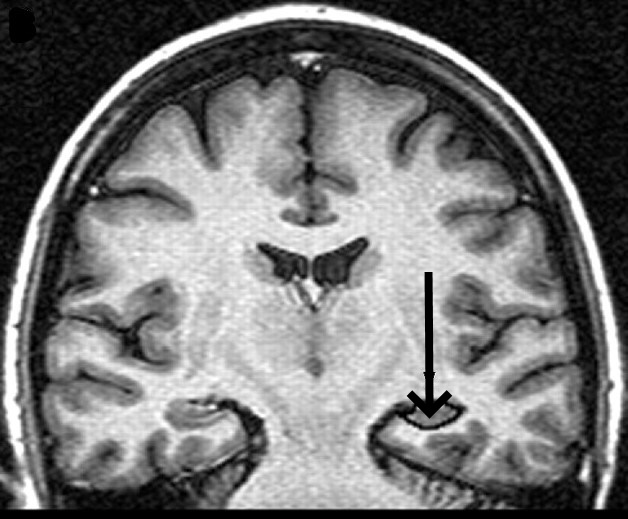
Presence of vascular lesions and atrophy of the hippocampus.
Presence of a decrease in volume (atrophy) in the hippocampus in a patient with subcortical frontal dementia.
The diagnosis of Alzheimer’s disease remains therefore uncertain.
Symptoms are those seen in subcortical frontal dementia.
The patient continues to receive an acetylcholinesterase inhibitor type medicine (e.g. Aricept) and a platelet aggregation inhibitor.
Semantic dementia, also called semantic variant primary progressive aphasia, is a type of frontotemporal dementia.
Others of frontotemporal dementia include frontotemporal dementia with behavioral variant and primary progressive nonfluid aphasia.
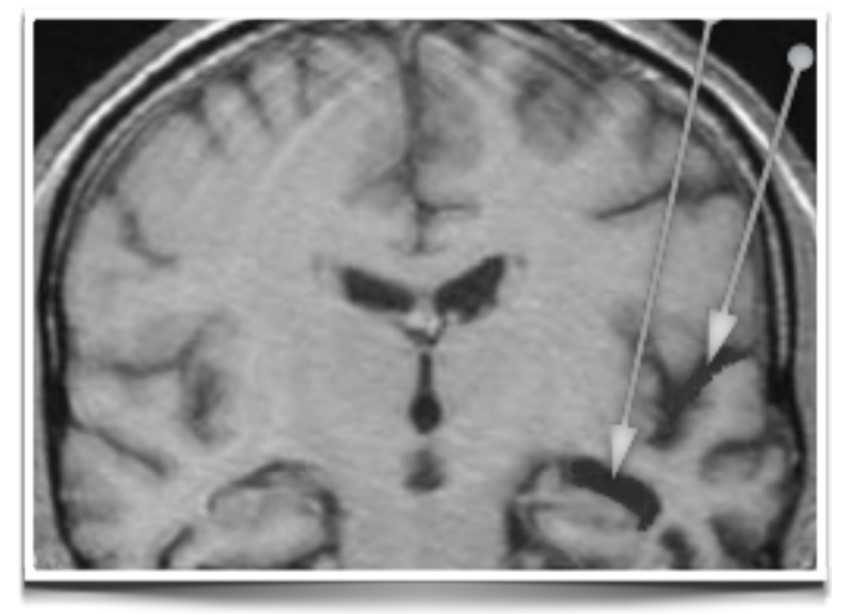
Left temporal atrophy (arrows) in a patient with semantic dementia
The pattern of disturbances in this form of dementia is different from that seen in more common dementias, such as Alzheimer’s disease, in which disturbances in recent memory, for example, are often an early symptom.
In contrast, in semantic dementia, recent daily memories and visuospatial function are relatively well preserved.
This means that people with this form of dementia are often able to recall recent events and can walk around their locality on their own without getting lost.
There are, however, significant changes in communication skills, personality, and behavior in semantic dementia.
The loss of semantic knowledge leads to difficulty finding words in conversation, including the names of people, places, and objects, as well as significant difficulty understanding the speech of others.
Semantic loss extends beyond language skills to affect nonverbal understanding of the world.
This leads to problems recognizing and understanding words, objects, faces, sounds, smells, touch and tastes, and causes challenges with activities of daily living.
Thus, sufferers may not be able to demonstrate how to use common items, such as a hammer or a comb.
Personality and behavioral changes are also common in this dementia, with behavioral characteristics having much in common with the behavioral variant of frontotemporal dementia in the later stages of the disease.
Mixed dementia is a disease in which abnormalities characteristic of more than one type of dementia occur simultaneously.
Doctors may also call mixed dementia « dementia – multifactorial. »
In the most common form of mixed dementia, the abnormal protein deposits associated with Alzheimer’s disease (amyloid proteins) coexist with blood vessel problems related to vascular dementia. Alzheimer’s brain changes often coexist with the Lewy body. In some cases, a person may have brain changes related to all three forms of dementia: Alzheimer’s disease, vascular dementia, and Lewy body dementia.
Researchers don’t know exactly how many older people currently diagnosed with a specific type of dementia actually have mixed dementia, but autopsies show the condition may be much more common than previously realized.
Autopsy studies play a key role in shedding light on mixed dementia because scientists cannot yet measure most dementia-related brain changes in living individuals.
In the most informative studies, researchers correlate any problem diagnosed during the participant’s lifetime with analysis of their brain after death.
In a study conducted in the United States, data from the first 141 volunteers showed that more than 50% of those whose brains met the criteria for Alzheimer’s disease also had at least one other type of dementia.
Symptoms of Mixed Dementia
Symptoms can vary depending on the types of brain changes involved and the brain regions affected.
In many cases, the symptoms may be similar or even indistinguishable from those of Alzheimer’s disease or another type of dementia. In other cases, a person’s symptoms may suggest the presence of more than one type of dementia.
Frontotemporal dementia is a form of dementia characterized by behavioral and language disorders associated with cognitive decline.
Clinicians distinguish between three forms of frontotemporal dementia based on the signs and symptoms that affect the individual:
Behavioral-variant frontotemporal dementia.
semantic dementia
Progressive non-fluent aphasia
Pick’s disease is also considered one of the forms of frontotemporal degeneration, manifested by changes in behavior: isolation, disinhibition, neglect of hygiene, distraction or continual repetition of the same gestures.
At first, frontotemporal dementia is mainly manifested by behavioral and language disorders that appear together or successively over time. They vary from patient to patient.
As it occurs remembered at a young age, it can be difficult to differentiate it from schizophrenia or an affective disorder.
Most often, behavioral problems predominate.
The majority of cases (about 70%) are sporadic (i.e. isolated cases with no hereditary form). There are therefore approximately 30% of familial cases of FTD which can be caused by at least four known genes (the tau and progranulin genes, and more rarely the VCP and CHMP2B genes).
Most often, the genetic anomaly seems to be transmitted autosomally (from generation to generation), which means that the patient has a risk in two of transmitting the disease to his children.
Prevalence of frontotemporal dementia
The prevalence (number of patients affected at a given time) of frontotemporal dementia varies between 3 and 15 cases per 100,000 people. It increases with age. Men seem to be more affected than women.
It is the 3rd cause of degenerative dementia. It represents 15 to 20% of the causes of dementia.
The age of onset is in the late 50s (range ages 20 to 75).
Life expectancy, from the moment of diagnosis, is on average about ten years.
Signs and Symptoms of Frontotemporal Dementia
1. Behavioral variant of frontotemporal dementia
This form affects about 60% of patients with one of the three forms of frontotemporal dementia.
The diagnostic criteria for this form are:
A. Progressive deterioration in behavior and/or cognition.
B. Three of the six behavioral/cognitive symptoms must be present. Rather, they must be persistent or recurring.
• Early disinhibition: inappropriate social behavior, loss of propriety or politeness and/or impulsive, thoughtless or even reckless acts. Disinhibition results in foul language, familiarity, or inappropriate attitudes (for example, they undress, behave badly at the table, urinate in public, etc.).
• Early apathy/inertia.
• Early loss of sympathy or empathy: diminished response to other people’s needs and feelings and/or social disinterest, impaired interpersonal relationships, emotional blunting.
• Early stereotyped or compulsive/obsessional behavior: simple repetitive movements, complex compulsive behaviors and/or verbal stereotypies: the patient repeats the same gestures, has fixed time habits, becomes fixated on certain objects or practices certain hobbies to excess such as the casino.
• Hyperorality and change in eating habits: changes in food tastes and/or gluttony, increased consumption of alcohol or cigarettes.
• Neuropsychological profile: executive function deficit and relative loss of episodic memory and visuo-spatial functions.
2. Semantic dementia
It concerns about 20% of cases and is mainly characterized by language disorders.
• Anomie-type disorders (difficulty finding words) despite preserved verbal fluency. For example, the person uses the word « bird » rather than « sparrow » or « thing, thing » rather than the appropriate word. Understanding is preserved.
• In more severe cases, the patient has problems identifying objects or animals. He can for example ask the following question: « What is a bird? » « . The person can, however, continue to manipulate numbers.
From an anatomical point of view, it is characterized by atrophy of the left temporal lobe.
3. Progressive non-fluent aphasia
It concerns about 20% of cases and is also characterized by language disorders. The person generally speaks slowly, has difficulty understanding the meaning of words, lacks verbal fluency, has great difficulty speaking on the telephone, expressing himself within a group or understanding complex sentences. Many of them develop Parkinson’s-like motor symptoms (for example, muscle rigidity in the arms and legs).
At the onset of the disease, memory impairment is minimal. Neuropsychological tests indicate that the information is well stored by the patient’s brain but that it has difficulty in being restored (for example, the patient does not retain such and such a word unless given a clue).
Fronto-temporal atrophy predominates in the left hemisphere, with a language disorder on expression, comprehension being relatively preserved.
Other Disorders
• Judgment and planning problems: patients cannot plan an activity.
• Swallowing disorders (severe stage of the disease).
Evaluation of frontotemporal dementia
The Frontal Dysfunction Scale assesses the severity of behavioral disturbances in patients with mild-stage dementia.
What brain imaging says
Unlike Alzheimer’s disease, which affects almost the entire brain, frontotemporal dementia preferentially affects the temporal lobe and the frontal lobe.
Neuroimaging techniques have made it possible to observe lesions of the frontal lobes (seat of reasoning, abstract ideas, planning, motor skills) and temporal (seat of the formation and retrieval of memories), and sometimes the lobes parietals.
In the late phase of the disease, there is significant neuronal loss in the cortex.
Magnetic resonance imaging (MRI) or CT scans are used to support a diagnosis of frontotemporal dementia.
Single photon emission computed tomography (SPECT) is an imaging technique that assesses the activity of the frontal and temporal lobes (in DFT, this activity is decreased).
These techniques do not make it possible to distinguish between the different forms of frontotemporal dementia. Detecting Pick’s bodies can only be done on post-mortem tissues (i.e. after autopsy).
Differential diagnosis
Frontotemporal dementia can be confused with many other neuropsychiatric diseases, especially early in the disease; eg depression, bipolar or obsessive-compulsive disorder), with a tumor of the frontal lobe, head trauma, certain infectious diseases, dementia associated with movement pathology or vascular dementia or chronic alcoholism.
Alzheimer’s disease is distinguished from frontotemporal dementia by early memory and orientation disorders marked from the onset of the disease.
Therapies
Medicines are prescribed in low doses at the beginning of treatment, before these are gradually increased according to possible side effects.
Antidepressants
Antidepressants are used to treat the following disorders:
• Anxiety and panic attack
• Obsessive Compulsive Disorder
• Aggressiveness
Selective serotonin reuptake inhibitors are the types of antidepressants of choice:
Antipsychotics are prescribed in low doses to reduce aggression, obsessive/compulsive disorder, irrational behavior with, however, undesirable side effects: weight gain, slowed thoughts, increased risk of heart disease. Atypical antipsychotics are the types of antipsychotics of choice: olanzepine (Zyprexa®), quetiapine (Seroquel® or Ketipinor®), risperidone (Risperdal®), ziprasidone (Geodon®), aripiprazole (Abilify®), paliperidone (Invega®). Memantine, a drug already used in moderate to severe forms of Alzheimer’s disease, would improve the memory function of patients with frontotemporal dementia.
Exercises
A training program combining aerobic (walking) and strength training is beneficial for the patient (for example the practice of cardiovascular exercises for 30 minutes 2 to 4 times a week, in the form of walking for example).
Clinical case
Mrs X, 79 years old, is being followed by a neurologist because she has mild cognitive deficits (mini mental state examination score of 26 out of 30). She was subsequently hospitalized for behavioral problems with periods of agitation and delusional disorders.
His entourage indicates that these behavioral changes appeared 4 years ago, with sometimes running away, compulsive shopping and a lack of social etiquette.
Treatment consisted of prescribing an antipsychotic (risperidone), a mood stabilizer (Valproate) and an antidepressant.
There is also a reduction in verbal fluency while episodic and visuo-spatial memories appear normal.
Neuroimaging reveals decreased activity in the frontal cortex and temporal lobe.
A diagnosis of frontotemporal dementia (degeneration) is made. His cognitive performance deteriorates with, in particular, a loss of language.
As a reminder, the symptoms of frontotemporal dementia are characterized:
In three quarters of cases by apathy, depression.
In a quarter of cases by mania, disinhibition (loss of social etiquette), hypersexuality and compulsive shopping.
Mild cognitive deficits at the onset of the disease (no memory loss).
Attention and executive function disorders.
Eating disorders (especially bulimia).
Treatment is limited to antidepressants and mood stabilizers.
Frontotemporal dementia linked to abnormal eating behavior
Patients with frontotemporal dementia have inappropriate eating habits.
While patients with the behavioral variant overeat (especially foods high in sugar) patients with semantic dementia (another form of frontotemporal dementia) exhibit very rigid eating behavior, sometimes focusing on a specific food .
Brain imaging has also suggested that these eating habits are controlled by complex neural networks rather than a particular brain structure.
Frontotemporal dementia (FTD) is the second leading cause of dementia occurring in people under the age of 65. There are several types of FTD: the behavioral variant which is manifested in particular by inappropriate behavior and an inability to plan, while semantic dementia is characterized by a loss of the meaning of words.
“It is possible that changing dietary habits may have a protective role in frontotemporal dementia. It is necessary to know if we can change these eating behaviors and if it will make a difference,” says the study’s lead author.
49 patients with three different types of dementia (19 with the behavioral variant, 15 with semantic dementia, and 15 with Alzheimer’s disease) participated in the study. Their eating habits were compared with those of 25 healthy controls.
All participants fasted overnight and then received a breakfast buffet. The researchers calculated the total amount and type of food eaten.
The results showed that all patients with the behavioral variant consumed more calories than the other participants, with an average of 1344 calories, compared to 710 calories for the Alzheimer group, 573 calories for the semantic dementia group and 603 calories for group control.
“Patients with the behavioral variant who ate the least even consumed more calories than those in the other groups who ate the most. »
In contrast, patients with semantic dementia showed rigid eating behavior, often refusing to eat the food offered.
The lead author (Dr. Ahmed) noted that sugar craving appears to be a particular feature of the behavioral variant of FTD.
It is possible that these patients have changes in their metabolism that could be the cause of the overeating.
The researchers also studied the participants’ brains (with the behavioral variant) using MRI to look for dysfunctions in specific areas of the brain. They found that overeating is associated with complex brain networks involved in reward, autonomic function, and vision, not specific brain structure.
Source: Rebekah M. Ahmed et al. Eating Disruption and Associated Eating Behavior Assessment of Neural Networks in Frontotemporal Dementia. JAMA Neurol. 2016; 73 (3): 282-290.
Patients with frontotemporal dementia have less emotion
An Australian study has shown for the first time why patients suffering from frontotemporal dementia have less emotion when faced with a memory. This explains why they feel no emotion when they remember a significant event (e.g. a wedding or a funeral). Professor Piguet, author of the study, says, “Until now, we knew that emotional memories were linked to the amygdala, a region of the brain involved in emotions. This study is the first to demonstrate the involvement of another structure, the orbitofrontal cortex, in this process. » Another researcher in the group, Fiona Kumfor, argues that these findings will help caregivers better understand why their sick loved ones may have difficulty interacting with them.
“Imagine attending your daughter’s wedding, or meeting your grandchild for the first time, but the event is as memorable as grocery shopping, says Dr. Kumfor. Source: The orbitofrontal cortex is involved in emotional enhancement of memory: evidence from the dementias. Brain, 2013.
Lewy body dementia is characterized by cognitive decline, visual and spatial disturbances, fluctuations in alertness and attention, hallucinations and motor disturbances.
Most cases of Lewy body dementia are sporadic. Some hereditary cases have been reported.
Historical
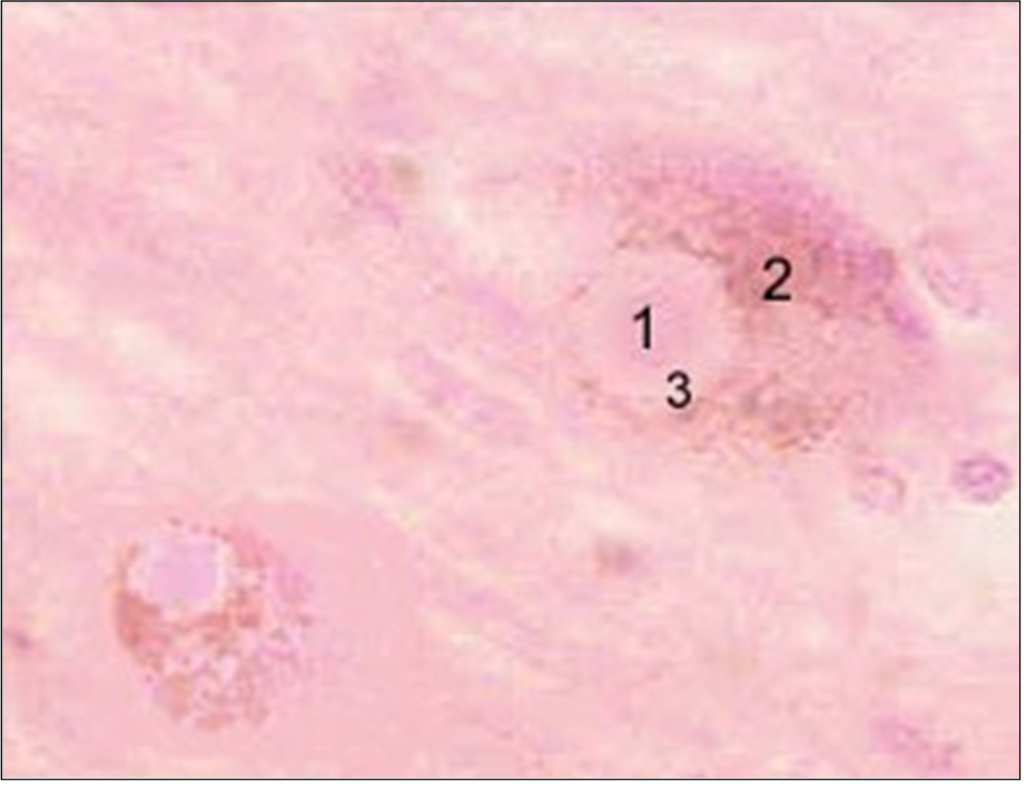
1912: the scientist Friederich Lewy observes for the first time ‘inclusions’ of about ten microns (one thousandth of a millimeter) in diameter, inside neurons. These inclusions, made up of deposits of proteins called alpha-synuclein, had previously been described in Parkinson’s disease. These inclusions are subsequently called Lewy bodies.
Lewy body (1) inside a neuron (2), stained pink with hematoxylin (a cytoplasm stain). The central part of the body of Lewy (1), of dense color, is surrounded by a halo, of pale color (3). The shape of Lewy bodies depends on their location. Thus, the Lewy bodies located in the cerebral cortex are devoid of halo, unlike those located in the brainstem.
1923: Friederich Lewy reports the existence of mental disorders in patients with Parkinson’s disease. He suggests the presence of ‘foreign bodies’ (later called Lewy bodies by Prof. Tretiakoff) inside neurons.
1961: Professor Okazaki reports the case of two patients with dementia associated with behavioral and motor disorders. The autopsy reveals the presence of Lewy bodies in the cerebral cortex.
1984: Pr Kosaka proposes the term Lewy body disease after collecting several cases of dementia patients. These patients presented with Lewy bodies in the brainstem and in certain regions of the temporal lobe related to the limbic system (anterior cingulate cortex, amygdala, and hippocampus).
1996: A group of researchers hold a conference to define diagnostic criteria for what is now called Lewy body dementia (abbreviated as LDB). LDB is therefore defined as a neurodegenerative dementia grouping the following terms: diffuse Lewy body disease, cortical Lewy body disease, Lewy body disease, senile dementia of the Lewy type, dementia with Lewy bodies, the variant with Lewy bodies of Alzheimer’s disease.
This working group revised the clinical and pathological diagnostic criteria and included new recommendations on how to better detect clinical symptoms.
Epidemiology
LDB accounts for 10% to 22% of post-autopsy dementia cases. By way of comparison, Alzheimer’s disease and vascular dementia account for 40-70% and 10-15% of dementia cases respectively. It is therefore the second leading cause of dementia.
The average age of onset is between 50 and 70 years, and affects more particularly men. A minority of MCI patients also have Parkinson’s disease. However, unlike patients with Parkinson’s, motor symptoms are usually mild and not accompanied by resting tremors. Most people with MCI have symptoms and lesions characteristic of Alzheimer’s disease.
Genetic factors
Most cases of LDB are sporadic, that is, affecting individuals irregularly. However, there are genetic mutations that can increase the risk of developing a sporadic form of the disease.
There are also family forms of the disease, explained by the mutation of genes (for example, the gene for alpha-synuclein).
Histological lesions of Lewy body dementia
Lewy bodies. These typical lesions contain proteins called alpha-synuclein and ubiquitin. These Lewy bodies are found inside neurons located in cortical (hippocampus, cingulate cortex, amygdala, basal nucleus of Meynert, hypothalamus) and subcortical (substance nigra, locus coeruleus, raphe nucleus, motor nucleus of vagus nerve) of the brain. The regions of the frontal cortex are less affected.
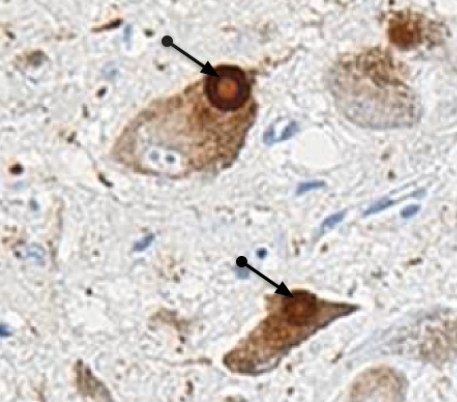
Lewy body (black arrow) inside a neuron. Post-mortem brain section from a patient with Lewy body dementia.
The presence of Lewy bodies in cortical regions seems to be related to the deterioration of intellectual functions.
Extensions of Lewy bodies are observed in the regions of the limbic system and the temporal lobe.
Lewy bodies and Alzheimer’s disease. A notable proportion of LDB patients present with lesions suggestive of Alzheimer’s disease: deposits of paired filaments in a helix (also called neurofibrillary tangles) and amyloid plaques. However, these filament deposits are less common in the brains of patients. According to the Braak scale, their number is between those of a healthy subject of the same age and that of an Alzheimer patient. On the other hand, the number of amyloid plaques is substantially identical in the two diseases, and appear more diffuse in LDB.
Lewy bodies and Parkinson’s disease. Lewy bodies are detected in the subcortical regions (substantia nigra and locus coeruleus) of brains of Parkinsonian patients.
Neuroimaging shows mild hippocampal atrophy in LDB compared to brains of healthy subjects. The activity of the primary visual cortex is reduced in patients with MCI.
Other types of lesions – called spongioses – appear in regions of the temporal lobe, particularly the tonsil.
Changes in neurotransmitters
The presence of these lesions in certain specific regions of the brain obviously has repercussions on the functioning of neurons.
Dementia with Lewy bodies is accompanied by a loss of neurons in the substantia nigra and the basal nucleus of Meynert, resulting in a decrease in the production of neurotransmitters called dopamine (DA) and acetylcholine (Ach), respectively.
Ach is the neurotransmitter of memory and attention, while DA is involved in motor control.
The death of neurons secreting Ach is probably responsible for cognitive disorders affecting in particular attention, concentration, visuo-spatial abilities, as well as visual hallucinations.
Motor disorders of the parkinsonian type are caused by a loss of neurons in the substantia nigra producing AD. Neuronal loss has also been described in the locus coeruleus, a region of the brain closely linked to the limbic system and synthesizing norepinephrine, an excitatory neurotransmitter. This neuronal death may be the cause of the behavioral disorders of paradoxical sleep observed in the disease.
Three main neural systems are therefore affected in LDB cholinergic (Ach), dopaminergic (DA) and noradrenergic (NA) systems.
The cholinergic system . Meynert’s basal nucleus contains neuron cell bodies (black circle) projecting to much of the cortex and the amygdala. These neurons synthesize acetylcholine, a neurotransmitter involved in memory storage and recall, motivation and attention. There is a significant loss of neurons from the basal nucleus of Meynert in DLB and Alzheimer’s disease (about two-thirds loss). The other acetylcholine-secreting nucleus is the septum (blue circle), whose neurons project into the hippocampus (blue arrow).
The dopaminergic system . The substantia nigra is made up of neurons (green circle) projecting into the striatum (a brain region involved in motor functions). These neurons synthesize dopamine and are particularly affected in DLB and Parkinson’s disease.
The noradrenergic system . The locus coeruleus (red circle), located in the brainstem, contains neurons projecting to the cortex, cerebellum and spinal cord (red arrows). These neurons synthesize norepinephrine, an excitatory neurotransmitter.
Clinical signs of Lewy body dementia
Clinical signs are characterized by both neurological, psychological and behavioral disorders, occurring insidiously and progressing over a period of several months to several years. The age of onset of LDB varies between 50 and 80 years. Men are slightly more affected than women.
According to the recommendations of the group of international experts, the essential criteria for the diagnosis of LDB are:
Progressive dementia, i.e. progressive cognitive decline severe enough to interfere with activities of daily living (domestic and social activities).
Predominance of visual and spatial disturbances (e.g. the patient no longer recognizes a route that he usually takes). Executive functions (reasoning, decision-making, abstract thinking, etc.) also decline. Visuospatial deficits are due to the presence of Lewy bodies in the visual associative cortex, located at the base of the temporal and occipital lobes. It should be noted that these lesions are not responsible for the slowing down of motor functions. The lack of perception is apparently at the origin of delusional disorders and misidentification (for example paramnesia, Capgras syndrome or the fact of not recognizing a relative). The patient also suffers from a significant attention deficit.
Memory problems (in particular verbal memory) which do not necessarily appear at the start of the disease, but which gradually worsen.
In addition to these main criteria, there are so-called secondary criteria. Two criteria are sufficient for the diagnosis of probable MCI, one criterion for the diagnosis of possible MCI).
Fluctuations in alertness and attention . These cognitive fluctuations are more marked and more frequent than in Alzheimer’s patients with a comparable cognitive deficit. They vary in duration and are similar to delusional disorders – they are sometimes called ‘pseudodelirium’. The characteristic signs are: loss of attention, incoherent language, hypersomnolence, impaired consciousness, staring into space. The patient suddenly returns to normal, confusing the family. The prevalence of fluctuations varies from 25 to 75%. Inexperienced physicians may have difficulty determining whether these fluctuations are secondary criteria for LDB.
A four-item questionnaire assesses the presence of these fluctuations with some precision. These items are:
the person is sleepy and has a lethargic behavior during the day, although he sleeps through the night,
she sleeps at least two hours during the day (before 7 p.m.),
she has a lost look for long moments and
sometimes disordered and confused thoughts.
This questionnaire detects with a high probability (positive predictive value* = 83%) the presence of DCL (and the absence of Alzheimer’s disease) if three of the four criteria are met.
Positive predictive value of a sign for a diagnosis: probability that the diagnosis is true if the sign is present.
Visual hallucinations recurrent and detailed, sometimes accompanied by auditory hallucinations. They are one of the cardinal signs of the disease, although they also appear in other forms of mental illness (Alzheimer’s disease, vascular dementia, hallucinatory psychosis). Hallucinations occur early in the disease and are persistent. They come in the form of innocuous three-dimensional images, representing people, animals or objects. Patients suffering from visual hallucinations early generally see their physical and mental condition worsen more quickly. A deficit of acetylcholine in the temporal lobe is probably responsible for these visual hallucinations. It should be noted that the associative visual cortex of the temporal lobe contains Lewy bodies.
Parkinsonian-like motor disorders. The vast majority of patients (up to 70%) show parkinsonian signs. These disorders are usually mild. They precede or follow the cognitive and behavioral disorders in a time interval not exceeding one year. If this is not the case, the doctor will make a differential diagnosis: other parkinsonian syndrome, dementia associated with Parkinson’s disease. Bradykinesia (slowness of body movements) is the main symptom. Gait disturbance, unsteady gait, limb stiffness and dystonia may occur as the disease progresses, or in response to treatment with antipsychotics (e.g. clozapine, risperidone) for soothe hallucinations. On the other hand, tremors at rest are rare.
Other criteria support the presence of a DLB:
Orthostatic arterial hypotension and postural instability, resulting in dizziness, fainting, transient loss of consciousness, with or without falls. Orthostatic hypotension with syncope is observed in a quarter of patients.
Hypersensitivity to antipsychotics (neuroleptics). Adverse effects suffered by patients with Lewy body dementia and treated with antipsychotics are frequent: sedation, rigidity, postural instability, falls and confusional state. The risk of mortality is doubled in patients treated with antipsychotics.
Oculomotor disorders.
Sleeping troubles. REM sleep (oneiric period of sleep) is characterized by muscle atony in healthy people. Patients with DLB develop REM sleep behavior disorders with violent shaking of the limbs during dream activity, excessive restlessness, persistent muscle tone, and absence of epileptiform electroencephalogram activity. The patient feels tired, but is usually unaware of this behavior. These disorders can be caused by cholinesterase inhibitors (eg Aricept, Exelon, Reminyl) prescribed for the treatment of cognitive disorders. Finally, a study has observed that these disorders can take years or even decades to dementia or Parkinson’s disease.
Depression. Depression and apathy are common and may be related to the severity of movement disorders.
Psychomotor restlessness.
Delusions, often elaborate.
Diagnostic criteria
Criteria
Essential criteria
Gradual cognitive decline, Persistent memory impairment, not necessarily early stage, Deficit in attention and visual/spatial ability.
Important signs of the disease
Cognitive fluctuations, Recurrent visual hallucinations, Parkinsonian-like motor symptoms.
Exclusion criteria
Presence of cerebrovascular disease (stroke, transient ischemic) validated by cerebral imaging, Parkinsonian symptoms occurring only in the severe stage of dementia.
These criteria make it possible to distinguish, with a small margin of error, a patient with MCI from a normal healthy subject (specificity* of the order of 80-100%). On the other hand, their sensitivity** is low and very variable (from 22 to 80%), suggesting that the prevalence of Lewy body dementia is underestimated.
It is estimated that an individual has an 80% risk of having MCI if they suffer from:
of progressive dementia
parkinsonian symptoms
visual hallucinations
The medical community emphasizes fluctuations in alertness and attention.
Differential diagnosis
The doctor will rule out the diagnosis of LDB and will suspect another pathology depending on whether the symptoms are dominated by motor disorders of the Parkinsonian type, a cognitive deficit with loss of autonomy, or psychological and behavioral disorders. The conditions close to LDB on which the doctor will pay particular attention are the following:
Alzheimer’s disease (AD). Disorders of episodic memory (recall of recent events) are earlier and more marked in AD than in DLB. Patients with Lewy body dementia, on the other hand, have a more impaired working memory, and more marked disturbances in attention, misidentification and delusional ideas. Visual hallucinations are observed later in AD. If the dementia appears more than a year before the onset of motor disorders, AD accompanied by a parkinsonian syndrome is preferred.
Vascular dementia. The cognitive disorders observed in vascular dementia depend on the location of the cerebral infarction, and are sometimes accompanied by an apathetic state and motor disorders. Cerebrovascular lesions are uncommon in LDB.
Parkinsonian type motor disorders. If the motor disorders precede the cognitive and behavioral disorders by more than a year, the presence of Parkinson’s disease or another form of parkinsonism is likely. Parkinson’s disease is likely if the patient suffers from tremors at rest and postural instability.
Other forms of parkinsonism can be considered such as:
Progressive supranuclear palsy, differing from LDB by a more marked gait disorder and the absence of delusional ideas. The patient also has oculomotor disorders.
Multiple system atrophy, which is very rarely accompanied by dementia. This parkinsonian syndrome is dominated by rigidity, akinesia (slow initiation of movements), and signs of dysautonomia (orthostatic hypotension, pupillary abnormalities, sphincter disorders).
Corticobasal degeneration: apraxic disorders are more pronounced than in Lewy body dementia. The motor signs (akinesia, rigidity) are very asymmetrical.
Creutzfeld-Jacob disease. Although the two diseases have common characteristics (abnormalities of the electroencephalogram, muscular contractions), the evolution of Creutzfeld-Jacob disease is generally fatal in less than a year. Analysis of the cerebrospinal fluid can help with the diagnosis, but only the autopsy can confirm it.
Schizophrenia. Also called hallucinatory psychosis, this is preferred if the hallucinations are both visual and auditory (for example the patient hears voices telling him to harm himself), and are accompanied by delusions without cognitive decline or disorder engine.
Metabolic dementia. Laboratory tests – blood tests, evaluation of thyroid function, blood levels of vitamin B12, brain imaging – will rule out or not vitamin B12 deficiency (often accompanied by psychosis), hypothyroidism (insufficient secretion of the thyroid resulting in psychomotor retardation, executive function disorders and psychosis). Cerebral imaging allows or not to eliminate the presence of lesions (lesions of the nuclei of the basal ganglia, of the thalamus and of the associative visual cortex) or cerebral anomalies (hydrocephalus, subdural hematoma) causing symptoms similar to those observed in Lewy body dementia. Imaging can also detect brain tumors affecting the lower temporal lobe and responsible for hallucinations and confusion. However, these tumors are rare.
Treatments of Lewy body dementia
Treatment of psychotic and behavioral disorders with antipsychotics is tricky because these patients are hypersensitive to this class of drugs.
This hypersensitivity aggravates the motor syndrome and induces states of acute agitation, leading to institutionalization.
Antipsychotics are the drug of choice, while limiting its dosage. Indeed, whether typical or atypical, they increase the risk:
death and stroke in older people with dementia. The risk factors are: age over 65, existence of sedation, malnutrition, dehydration, lung disease or concomitant treatment with benzodiazepines.
fall, this risk being already present in the Lewy body dementia.
They could also aggravate the cognitive deficit by promoting the appearance of lesions characteristic of Alzheimer’s disease (deposits of amyloid and neurofibrils).
Rivastigmine, a drug prescribed for cognitive disorders in Alzheimer’s disease, seems to reduce neuropsychiatric symptoms (eg delirium) in MCI and improve the quality of life of these patients.
Clinical case
An 80-year-old patient was hospitalized in a psychiatric unit for behavioral disorders (aggressiveness, confusional state) following treatment with an antipsychotic.
This person was previously diagnosed with dementia associated with a motor syndrome with:
cognitive disorders: temporal, gnostic and practical spatial disorders;
motor disorders: frozen face, voice and swallowing disorders, difficult walking.
He had been receiving rivastigmine and piribedil (a dopaminergic agent) for a year.
Despite the discontinuation of the antipsychotic treatment (replaced by an anxiolytic), the patient continued to exhibit agitation. Another anxiolytic was prescribed along with low-dose clozapine treatment. The gait disturbances were rapidly reduced, as well as his psychotic disturbances (hallucinations, agitation, aggressiveness).
Communication disorders in patients with dementia are increasingly present as the disease progresses, due to language and behavioral disorders. Factors favoring communication include the bringing into play of emotions, the application of body care and a good relationship between the patient and those around him.
Language is affected
Dementia is a disease of communication and, above all, of verbal communication. Indeed, the progression of the disease inevitably impoverishes the capacities of verbal exchange of the patient with his entourage. The real communication difficulties will mainly arise in the severe stage of his illness.
Verbal communication with the patient suffering from a cognitive function deficit is all the more difficult as the extent of the cerebral lesions – in particular the language areas – is marked. This deficit concerns:
comprehension disorders;
oral expression disorders dominated by a lack of words;
frequent paraphasias : words are distorted or substitute for others;
a simplification of the syntax;
in the most severe cases, the language becomes jargon with numerous neologisms.
Communication aggravating factors
Whether it is a family or medical environment, several factors can aggravate the exchange:
lack of availability, attention and listening. For example caregivers, who during a treatment, have a personal conversation from which the patient is excluded;
precipitation: the patient needs time to gather his ideas, find the right words and check that he has been understood. Otherwise, he will often prefer to be silent;
the medical jargon sometimes used by caregivers;
a statement by the patient considered uninteresting;
a failure at the start of a relationship where too much is asked of him, where he feels devalued.
How to optimize communication
Any cognitive stimulation can be conducive to inducing speech, especially in the case of sessions with a speech therapist. Other therapies (music therapy, relaxation techniques, art therapy) facilitate communication by strengthening self-esteem. Pleasant body treatments such as massages or cosmetic treatments can encourage the patient to talk.
How to stimulate the patient’s attention and motivation
Communication should never be forced. Caregivers to create a climate of trust and stimulate attention and motivation. For this it is necessary to:
go to a quiet place to create together a common space of exchange;
face the sick at the same level as him;
stimulate his attention by touch and gaze;
make simple sentences containing only one idea at a time;
say ‘I’ and avoid using ‘we’ which is too vague and impersonal;
ask questions to elicit ‘yes’ or ‘no’ answers, not ask for choices;
reformulate the patient’s words if necessary to check their content;
possibly help him find the missing words.
Patients suffering from dementia have a verbal expression that becomes more and more difficult. However, until the advanced phase of the disease, before the stage of mutism, the majority of them seek communication to express their experience, to speak in pairs, etc. When the verbal mode of communication disappears, the word is always possible, especially if a favorable climate favors it. Furthermore, It is necessary that the entourage is convinced that exchanging with them makes sense and that their words make sense.