Amyloid is a soluble protein that is normally eliminated in healthy people.
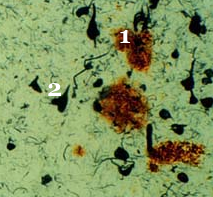
In people with Alzheimer’s, this protein becomes insoluble and agglutinates outside neurons to form amyloid (or senile) plaques (30 to 100 microns in diameter). This accumulation affects certain parts of the brain.
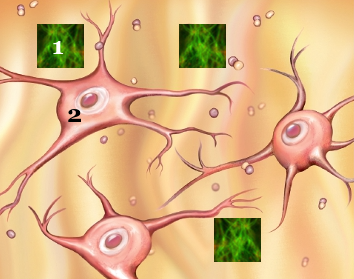
Beta-amyloid comes from a larger protein found in the membrane surrounding healthy nerve cells. Most researchers believe that the accumulation of amyloid protein is the cause of the neuronal death seen in Alzheimer’s disease. Other scientists think it is a consequence of the disease.
Amyloid really the cause of Alzheimer’s disease ?
Many researchers have argued that the buildup of amyloid in the brain causes Alzheimer’s disease. However, a new study published in 2020 contradicts this hypothesis.
Researchers have argued that beta-amyloid plaques disrupt communication between brain cells, which can lead to cognitive function problems.
This study published by a group of researchers from the University of California, San Diego suggests that while amyloid buildup is associated with Alzheimer’s disease, it may not cause the disease.
In this article published in the journal Neurology, the researchers explain what led them to this conclusion.
« The scientific community has long believed that amyloid causes the neurodegeneration and cognitive impairment associated with Alzheimer’s disease, » says lead author Professor Mark Bondi.
In their study, the researchers worked with a total of 747 participants with varying levels of cognitive health.
All study participants agreed to undergo neuropsychological assessments, as well as neuroimaging exams (PET and MRI brain scans ).
Of the participants, 305 were in good cognitive health, 289 had mild cognitive impairment, and 153 had markers of what the researchers call « objective subtle cognitive difficulties (Obj-SCD). »
Objective subtle cognitive difficulties define them as « difficulties on certain sensitive cognitive tasks even if the overall neuropsychological profile is within the norms ».
Previous research has suggested that people with Obj-SCD are at a higher risk for mild cognitive impairment and forms of dementia.
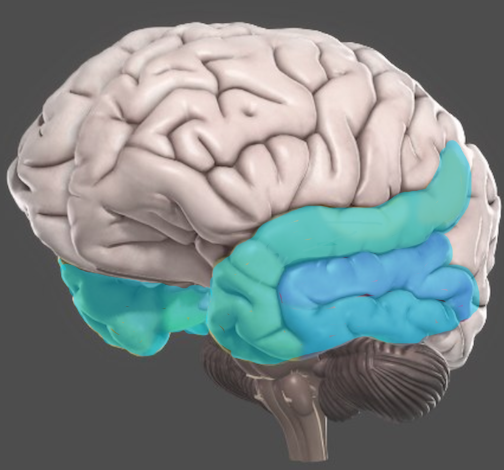
The researchers found that amyloid accumulated faster in participants with Obj-SCD than in those considered cognitively healthy. Additionally, brain scans of people with Obj-SCD showed that these people had experienced thinning of brain material in an area called the entorhinal cortex.
Previous research has shown that the entorhinal cortex decreases in size in people with Alzheimer’s disease. This is important because this brain region plays a role in memory and spatial orientation.
The researchers also found that while people with mild cognitive impairment had higher amounts of amyloid in their brains at the beginning of the study, this protein did not appear to build up any faster in these participants than in individuals that are not cognitively impaired.
But why do the current findings potentially contradict a decades-old hypothesis about the development of Alzheimer’s disease? Professor Bondi explains:
This work suggests that cognitive changes can occur before significant levels of amyloid have built up.
It seems that we need to focus on treatment targets for conditions other than amyloid, such as tau, which are more strongly associated with difficulty in thinking and remembering.