Découvrez comment jouer aux jeux de casino qui vous intéressent le plus, du Blackjack à la Roulette en passant par le poker, les machines à sous et plus encore.
Comprendre les règles de chaque jeu
Connaître les bases des jeux de casino est essentiel pour assurer une expérience de casino réussie. Avant de placer vos paris, il est important de comprendre les règles et le fonctionnement de chaque jeu. Bien que les principes de chacun soient similaires, vous aurez besoin de connaître des stratégies, des têtes hautes et des paiements spécifiques pour chaque variété. Cet article peut vous donner une idée sur l’intérêt que chaque jeu offre et augmenter vos chances de gagner.
Apprenez quelques stratégies de base pour gagner
Peu importe le jeu auquel vous décidez de jouer, vous pouvez suivre certaines stratégies de base. Par exemple, si vous jouez au blackjack, il est important de savoir quand tirer et rester en fonction de la valeur totale de votre carte par rapport à la carte révélée par le croupier. À la roulette, comprendre la différence entre la roulette américaine et européenne vous aidera également à augmenter vos chances. Avoir une stratégie claire peut être l’élément d’avantage dont vous avez besoin pour vous démarquer dans le jeu de casino de votre choix.
Fixez-vous des limites et respectez-les
N’oubliez pas que le jeu doit toujours consister à s’amuser et jamais à essayer de devenir riche. C’est pourquoi il est si important d’avoir des directives financières claires lorsque vous jouez à ces types de jeux. Avant de vous asseoir à l’une des tables, vous devez décider avec combien d’argent vous pouvez vous permettre de jouer, établir vos pertes maximales et fixer des limites de temps pour votre jeu. Assurez-vous de respecter ces limites et évitez autant que possible de courir après les pertes.
Utilisez les ressources en ligne pour rechercher des jeux et leur biologie
En savoir plus sur les différents types de jeux de casino et comprendre les probabilités qui les accompagnent peut être intimidant, même pour le joueur le plus expérimenté. Pour vous assurer que vous avez une meilleure compréhension du jeu, vous devriez envisager de faire des recherches en ligne. Des sites comme mr bet proposent des tutoriels approfondis et des critiques de jeux de casino populaires comme le blackjack, la roulette, le baccarat et le pai gow afin que vous puissiez comprendre les règles de chaque jeu avant de jouer. Faire des études sur la stratégie de jeu et le style de jeu peut vraiment vous aider à augmenter vos chances de gagner gros.
Profitez des jeux de casino gratuits en ligne pour pratiquer vos stratégies avant de jouer pour de l’argent
Avant de vous plonger dans le jeu en argent réel, il est important de vous entraîner à jouer à divers jeux de casino. En profitant des jeux de casino gratuits en ligne, vous pouvez perfectionner vos compétences et essayer de nouvelles stratégies dans un environnement sans risque. Même après avoir maîtrisé les règles d’un jeu, il est toujours essentiel de se familiariser avec tous les aspects du jeu avant de parier de l’argent réel dessus. Avec les jeux de casino gratuits disponibles en ligne, vous pouvez vous entraîner autant que vous le souhaitez jusqu’à ce que vous acquériez la confiance nécessaire pour réussir au jeu.
Êtes-vous prêt à votre soirée casino ? Si jouer à des jeux de cartes conventionnels commence à devenir ennuyeux, il existe de nombreux autres jeux de casino sans cartes qui peuvent ajouter du plaisir et de l’excitation ! Voici quelques choix pour les jeux de casino en ligne qui n’utilisent pas de cartes.
Roulette
Tentez votre chance au classique favori, la roulette ! Choisissez vos numéros porte-bonheur et pariez sur le résultat de la rotation de la roue. Si vous devinez correctement, vous recevrez un paiement en fonction du degré de risque (ou de sécurité) de votre pari !
Bingo
Le bingo est le jeu parfait pour les débutants comme pour les joueurs chevronnés ! Tentez votre chance en appelant les numéros au fur et à mesure qu’ils sont sélectionnés et cochez ceux qui pourraient apparaître sur votre billet. Obtenez-en assez pour former un motif et vous serez gagnant ! Pourriez-vous être le prochain grand gagnant ?
Machines à sous
Les machines à sous sont un jeu classique qui existe sous une forme ou une autre depuis des siècles. Pour jouer, insérez simplement des pièces dans la machine et appuyez sur le bouton Spin. En regardant les rouleaux tourner, vous espérerez faire la bonne combinaison de symboles et gagner gros ! Avec des machines de haute technologie offrant de nos jours des graphismes époustouflants, des effets sonores réalistes et des scénarios captivants, il n’est pas étonnant qu’ils restent si populaires auprès des joueurs.
Baccara
Le baccarat est un jeu de casino facile à apprendre et rapide à jouer. Battez simplement le banquier en vous rapprochant le plus possible de neuf. Il n’est pas étonnant que nous ayons vu le baccara dans des livres et des films tels que James Bond – c’est vraiment un jeu passionnant rempli d’adrénaline. Vous pouvez même jouer au baccara en direct en ligne avec un vrai croupier – le mélange parfait d’action de casino classique sans avoir à quitter la maison. Alors pourquoi ne pas essayer ?
Vidéo Poker
Le vidéo poker est l’un des jeux de casino sans cartes les plus populaires. Il combine des éléments du poker classique et des machines à sous. Vous commencez par mettre vos jetons dans la machine, puis sélectionnez le nombre de pièces avec lesquelles vous souhaitez jouer ainsi que le nombre de lignes que vous couvrirez. Alors c’est parti pour les courses ! Le vidéo poker commence comme un jeu normal de poker à cinq cartes – au lieu de jouer contre d’autres joueurs, vous êtes en compétition contre la machine. Essayez de faire votre meilleure main possible pour des prix en argent !
La Formule 1 est un sport qui déchaîne les passions depuis les débuts des sports mécaniques et le Grand Prix de France est riche de victoires et d’émotions intenses. Depuis ses débuts officiels en 1950 sur le circuit de Reims-Gueux, ce championnat a vu passer des champions mémorables sur des circuits de légende. Retour sur le Grand Prix de France avec des dates clés.
Les sports automobiles existent depuis la fin du 19e siècle, mais c’est bien le 2 juillet 1950 qu’on assiste au premier Grand Prix de France, avec la victoire de Fangio, pilote de légende dans sa Ferrari. À l’époque, les technologies utilisées pour faire fonctionner les machines sont encore balbutiantes, mais les grands pilotes savent gérer des courses de plus de deux heures.
La F1 devient populaire pour les sports betting in Canada. Cependant, il est pourtant difficile pour la compétition de s’imposer sur l’ensemble des circuits français à cause des exigences mécaniques de la Formule 1. Pour cette raison, le circuit des 24 heures du Mans n’accueillera plus jamais de Grand Prix après un Grand Prix compliqué en 1967.
Dans les années 70, les Formule 1 deviennent des monstres de puissance qui affichent rarement moins de 200 km/h en moyenne. Lorsque le circuit de Charade en Auvergne est utilisé pour un Grand Prix, le pilote Helmut Marko reçoit une pierre en plein visage et perd la vue d’un œil. Cet évènement marque la fin de ce circuit pour les compétitions de Formule 1.
Les années 80 sont marquées par la domination d’Alain Prost, champion français qui cumule 51 victoires de Grand Prix au long de sa carrière. Cette décennie de succès est couronnée en 1989 lorsque le Français remporte la 38e édition du GP sur le circuit Paul Ricard.
Le Grand Prix de F1 est marqué par l’immense Michael Schumacher qui règne sur la discipline dans tous les pays du monde. La France ne fait pas exception puisqu’il y remporte pas moins de cinq titres du Grand Prix de France, avant son dramatique accident de ski qui mit une fin brutale à sa carrière en 2013.
Les grands champions du Grand Prix de France
Parmi les pilotes français qui ont marqué la compétition, nous avons déjà cité Alain Prost, surnommé Le Professeur, un sportif exceptionnel dont le nombre de victoires en Grand Prix dépasse largement celui d’autres Français.
Comment ne pas citer Jean Alesi qui, malgré son faible nombre de victoires, est resté l’un des cadors de la F1 dans les années 90 ? C’est peut-être le manque de fiabilité moteur de ses machines ou sa mauvaise gestion émotionnelle qui expliquent en partie son manque de victoire.
René Arnoux fait partie d’une époque bénie où les F1 se lançaient à plus de 290 km/h avec à leur bord des pointures comme Jacques Lafitte, Alain Prost et Patrick Tambay. Avec sept victoires de Grand Prix avec la prestigieuse écurie Ferrari, nous nous souvenons particulièrement d’un duel mythique avec Gilles Villeneuve qui a montré au monde son sang froid et son impressionnante maîtrise du volant.
Le saviez-vous ?
S’il y a bien un geste emblématique qui vient à l’esprit lorsque l’on parle de Grand Prix, c’est la douche de champagnes qui a lieu sur les podiums après une victoire. L’origine de cette tradition propre à la Formule 1 nous vient depuis 1966, où le Suisse Jo Siffert a accidentellement arrosé la foule avec une énorme bouteille de Moet et Chandon. La bouteille n’était pas fraîche et le bouchon démuselé a sauté dans la foule en délire.
L’histoire du Grand Prix s’écrit au futur
Les nouveaux talents français sont bien là, avec la victoire d’Esteban Ocon sur le Grand Prix de Hongrie en 2021. Reste à savoir si le parcours du jeune espoir français s’inscrit dans la lignée des plus grands.
Genotropin de Pfizer est une hormone de croissance recombinante. Il est synthétisé par génie génétique. Ce médicament est fabriqué par Pfizer, une société pharmaceutique mondialement connue. Il a une bonne réputation auprès des sportifs. Les athlètes l’utilisent comme agent anabolisant. Aide à catalyser la lipolyse. Il a un effet complexe sur la composition en protéines, en glucides et en minéraux du corps humain. Stimule la croissance musculaire, accélère la combustion des graisses, rend le corps plus tolérant aux fortes contraintes physiques et aide à prévenir les blessures sportives.
Effet de la prise de Genotropin
Genotropin de Pfizer a fait ses preuves non seulement en médecine, mais aussi dans le sport. Des études ont montré que la somatropine a un effet positif sur le taux de lipolyse dans les dépôts graisseux sous-cutanés et le tissu viscéral, qui contient également de la graisse. Les effets suivants se produisent lors de la prise de ce médicament :
une augmentation de la concentration de HDL;
Diminution des niveaux de LDL.
La réalisation de l’effet anabolisant est due aux processus d’hypertrophie et d’hyperplasie se produisant dans les muscles. Étant donné que le prix de Genotropin est dans certains cas inférieur à celui d’autres médicaments similaires, il est souvent acheté pour obtenir l’effet d’augmentation de la synthèse des protéines et de l’activation des cellules souches. Ces derniers, une fois leur croissance et leur différenciation terminées, vont fusionner avec les fibres musculaires existantes.
Régime de génotropine pour les athlètes
Un cycle de GH convient aux hommes et aux femmes de plus de 20 ans. Cela est dû à la possibilité d’une croissance osseuse asymétrique chez les jeunes. Aide à développer de meilleurs muscles.
Avant de commander Genotropin, vous devez déterminer la quantité de médicament dont vous avez besoin par cours pour obtenir le résultat souhaité. Les spécialistes recommandent de ne pas prendre plus de 4000 UI de Genotropin par semaine et la période de prise ne doit pas dépasser 3 à 6 mois.
Quant à la fréquence d’administration, les culturistes utilisent environ 1000-1500 UI tous les 2 jours. Il convient de garder à l’esprit que les scientifiques ont trouvé le schéma suivant : une injection de 1500 UI entraîne une augmentation d’environ 300 % de la testostérone plasmatique et son niveau est maintenu jusqu’à 6 jours. Par conséquent, il est recommandé de faire les injections un peu moins fréquemment – 1 dose tous les 3-4 jours.
Combiner thérapie et médicaments peut être un moyen efficace de gérer les troubles mentaux, mais il peut également être difficile de comprendre comment ils devraient fonctionner ensemble.
Nous expliquerons pourquoi les thérapies et les médicaments peuvent être utiles, les avantages et les inconvénients de les combiner et des conseils pour tirer le meilleur parti du traitement.
Comprendre les rôles de la thérapie et des médicaments
La thérapie et les médicaments ont tous deux un rôle précieux à jouer dans le traitement de la santé mentale. Pour de nombreuses personnes, parler de leurs difficultés avec un thérapeute peut fournir un aperçu inestimable des causes de leurs symptômes et les aider à trouver des stratégies efficaces pour les gérer.
Pendant ce temps, les médicaments peuvent être utiles pour soulager les symptômes, alors que la thérapie s’attaque à la cause sous-jacente.
Recherchez des thérapeutes
Lorsque vous envisagez une combinaison de thérapie et de médicaments, il est important de trouver un thérapeute qui est à l’aise pour discuter du rôle des médicaments.
Envisagez d’en rechercher un qui a de l’expérience dans les deux domaines, comme un psychologue ou un psychiatre qui offre une thérapie par la parole ainsi que la gestion des médicaments.
Avoir quelqu’un qui comprend les deux aspects du traitement peut être inestimable lorsque vous travaillez à l’élaboration d’un plan complet de gestion de votre santé mentale.
Efficacité clinique
Le traitement des problèmes de santé mentale tels que la dépression, les troubles anxieux, les troubles liés à l’utilisation de substances, les troubles de l’alimentation, la schizophrénie ou le trouble bipolaire implique généralement une combinaison thérapie et médicaments.
La thérapie cognitivo-comportementale, la psychothérapie interpersonnelle et les antidépresseurs sont couramment utilisés pour traiter la dépression, tandis que la thérapie cognitivo-comportementale et d’autres thérapies sont utiles pour traiter les troubles anxieux.
Pour les problèmes de toxicomanie, la thérapie cognitivo-comportementale est la plus efficace combinée à la participation à un programme de soutien en 12 étapes. Le traitement des troubles de l’alimentation peut nécessiter une prise en charge médicale pour maintenir la sécurité physique et peut impliquer une psychothérapie en association avec des antidépresseurs.
Les médicaments antipsychotiques ou les stabilisateurs de l’humeur sont généralement prescrits pour traiter la schizophrénie ou le trouble bipolaire, mais les recherches suggèrent que l’ajout d’une psychothérapie cognitivo-comportementale ou familiale peut aider à améliorer les résultats fonctionnels.
La psychothérapie est généralement recommandée pour aider à résoudre les difficultés parentales, les problèmes de mariage ou les problèmes d’adaptation. La thérapie peut aider à développer des compétences et à mieux réagir aux facteurs de stress.
Trouvez des moyens de surveiller vos progrès avec la combinaison thérapie-médicaments
La partie délicate de la combinaison de la thérapie et des médicaments consiste à trouver le bon équilibre entre eux. Les deux approches ont leur propre efficacité et il est important de trouver des moyens de suivre vos progrès avec les deux.
Par exemple, vous pouvez suivre tout changement dans les sentiments ou les comportements par le biais d’un journal de bord et consulter régulièrement votre médecin et psychologue pour discuter de l’évolution. Cela les aidera à mieux comprendre ce qui fonctionne, ce qui ne fonctionne pas et comment ils peuvent soutenir vos objectifs.
Discutez de tous les effets secondaires avec votre professionnel de la santé
La combinaison de la thérapie et des médicaments peut entraîner de nombreux effets secondaires, notamment des symptômes physiques tels que des maux de tête, des nausées ou des troubles du sommeil. Il est important de parler à votre professionnel de la santé de tout effet secondaire que vous ressentez afin qu’il puisse ajuster la posologie ou l’approche si nécessaire.
Alternativement, si les effets secondaires sont suffisamment graves pour interférer avec le fonctionnement quotidien, les médicaments peuvent ne pas convenir et il peut être conseillé d’envisager d’autres traitements non médicamenteux à la place.
Consacrez du temps pour continuer à vous améliorer
Avant de commencer à combiner thérapie et médicaments, il est important de comprendre que les progrès ne se font pas du jour au lendemain.
Consacrez du temps chaque jour à améliorer votre santé mentale. Cela pourrait inclure des activités telles que l’exercice, le yoga, la prière ou les pratiques de pleine conscience. De plus, il est essentiel de se rappeler que le maintien d’une relation étroite avec votre thérapeute et votre médecin peut vous aider à vous assurer que vous recevez les meilleurs soins possibles.
Combining therapy and medication can be an effective way to manage mental disorders, but it can also be confusing to figure out how they should work together. Here, we’ll explain why both therapies and medications can be useful, the pros and cons of combining them, and tips for making the most of your treatment plan.
Understand the Roles of Therapy and Medication.
Therapy and medication both have valuable roles to play in mental health treatment. For many people, talking through their struggles with a therapist can provide invaluable insight into the causes of their symptoms and help them find effective strategies for managing them. Meanwhile, medications may be helpful in providing relief from symptoms while therapy works to address their underlying cause.
Look for Complementary Therapists.
When considering a combination of therapy and medication, it’s important to find a therapist who is comfortable discussing the role of medication. Consider looking for one that has experience in both fields, such as a psychologist or psychiatrist who provides talk therapy as well as medication management. Having someone who understands both aspects of treatment can be invaluable as you work to develop a comprehensive plan for managing your mental health.
Clinical evidence
Treatment for mental health challenges such as depression, anxiety disorders, substance use disorders, eating disorders, schizophrenia or bipolar disorder typically involves a combination of psychotherapy and medication.
Cognitive-behavioral therapy, interpersonal psychotherapy and antidepressants are commonly used to treat depression, while cognitive-behavioral therapy and other environment-based therapies are useful for treating anxiety disorders.
For substance abuse problems, cognitive-behavioral therapy is though to be most effective combined with participation in a 12-step support programs. Eating disorder treatment may require medical management to maintain physical safety and may involve psychotherapy in combination with antidepressant medications.
Antipsychotic medications or mood stabilizers are usually prescribed to treat schizophrenia or bipolar disorder but research suggest the addition of cognitive-behavioral or family psychotherapy can help improve functional outcomes.
Psychotherapy is typically recommended to help with parenting difficulties, marriage issues or adjustment concerns. Therapy can help build skills and respond better to stressors.
Find Ways to Monitor Your Progress with Both Options.
The tricky part of combining therapy and medication is finding the right balance between them. Both approaches have their own efficacy and it’s important to find ways to monitor your progress with both. For example, you can track any changes in feelings or behaviors through regular logs or journaling and check-in with your care team regularly to discuss these progress notes. This will help them better understand what’s working, what isn’t, and how they can support your mental health goals.
Discuss Any and All Side Effects with Your Medical Professional.
Combining therapy and medications can result in many side-effects, including physical symptoms like headaches, nausea, or trouble sleeping. It’s important to talk to your medical professional about any side effects you experience so that they can adjust the dosage or approach if necessary. Alternatively, if the side effects are severe enough to interfere with daily functioning then medication may not be suitable, and it might be advisable to consider other non-medicinal treatments instead.
Dedicate Time to Continue Improving Yourself and your Mental Health.
Before you begin to combine therapy and medication, it is important to understand that progress doesn’t happen overnight. Dedicate the time each day to improve your mental health. This could include activities such as journaling, exercise, yoga, or mindfulness practices. Additionally, it is key to remember that keeping a close relationship with your therapist and doctor can help ensure that you are getting the best care possible.
Animal therapy is an emerging field that has yielded positive results in treating physical and mental health issues. Through companionship, comfort, and physical contact, animals can provide support to those who may not be able to access other therapy options.
Definition and Types of Animal Therapy.
Animal therapy, also known as pet therapy, is defined as the use of animals for the purpose of improving physical, emotional and psychological health. There are three main types of animal therapy including anim-assisted psychotherapy, human-animal interaction therapy, and animal-assisted activities. Anim-assisted psychotherapy is focused on resolving a specific issue or problem usually through conversation and interaction with an animal therapist. Human-animal interaction therapy refers to the use of animals to create connections between humans by providing comfort and companionship. Animal-assisted activities provide companionship to people with disabilities or other limitations who may not be able to care for their own pets but need therapeutic contact with animals.
Benefits of Animal Therapy.
Studies have shown that animal therapy can reduce stress, provide emotional support, lower blood pressure and increase feelings of well-being. Interacting with an animal has been found to improve the morale and self-esteem of people suffering from depression, anxiety or other mental health issues. Animals also help to alleviate loneliness, build trust and motivate individuals to take part in various activities they may not be able to do on their own. Animal therapy can also aid in physical rehabilitation as working closely with animals helps individuals focus on something else, providing distraction from pain or discomfort.
Indications
Animal-assisted therapy can be beneficial for people with a variety of physical and emotional issues, including mental health issues such as depression and anxiety, physical disabilities, chronic pain, autism spectrum disorders and more. It is also used for patients facing terminal illnesses or end-of-life issues, as well as to comfort those in the hospital setting who may feel isolated or lonely. Furthermore, it can be used to help individuals suffering fromposttraumatic stress disorder (PTSD)or traumatic experiences.
Posttraumatic stress disorder
Animal therapy is on the rise as a legitimate form of treatment for posttraumatic stress disorder (PTSD). Research has found evidence suggesting that it can be beneficial to PTSD sufferers. In one study, it was observed that interacting with a dog for around a week caused an 82% reduction in symptoms. In addition, the amount of anxiety and sleep medications required by the patient in this particular case decreased by half. Clearly, incorporating animals into the traumatic experience can have a positive impact on those struggling with PTSD.
Considerations for Animal Therapy in Different Settings
Animal-assisted therapy can be implemented in a variety of settings including counseling centers, nursing homes, rehabilitation facilities, and schools. It is important to consider which type of animal and training is most suitable for the setting. For instance, puppies or small animals are great for children while medium or large dogs may be more appropriate in hospital settings. Ensure that the animal you choose has undergone proper training as this will make sure that it behaves appropriately in different environments.
Benefits in the elderly population
Animal assisted therapy is an evidence-based practice that utilizes pet interaction and animal related activities to boost physical and mental wellbeing. Recent studies have shown that this therapeutic intervention can result in a significant improvement in quality of life when experienced by older adults. This was determined through a meta-analysis with a sample size of 375 people, half in the experimental group and the other in the control group. The therapy sessions lasted around 38 minutes on average, with trials being performed between April – June of 2021.
Education and Training for Providers of Animal-Assisted Interventions
Providers of animal-assisted interventions must be educated about the appropriate selection and management of therapy animals, understand the scientific evidence for their effectiveness, recognize the principles of humane care, and possess skills to collaborate with individuals, families, and other professionals. Moreover, it is important that providers understand the importance of planning specific therapeutic activities related to each case. This can involve utilizing toys, games, and techniques (i.e., grooming) that stimulate physical interaction with the animal to increase relaxation or emotional connectedness.
Neurons (or nerve cells), fundamental units of the brain and nervous system, have different types and morphologies.
Neurons are the basis of the functioning of the brain. They are surrounded by non-neuronal cells called glial cells .
The different parts of neurons
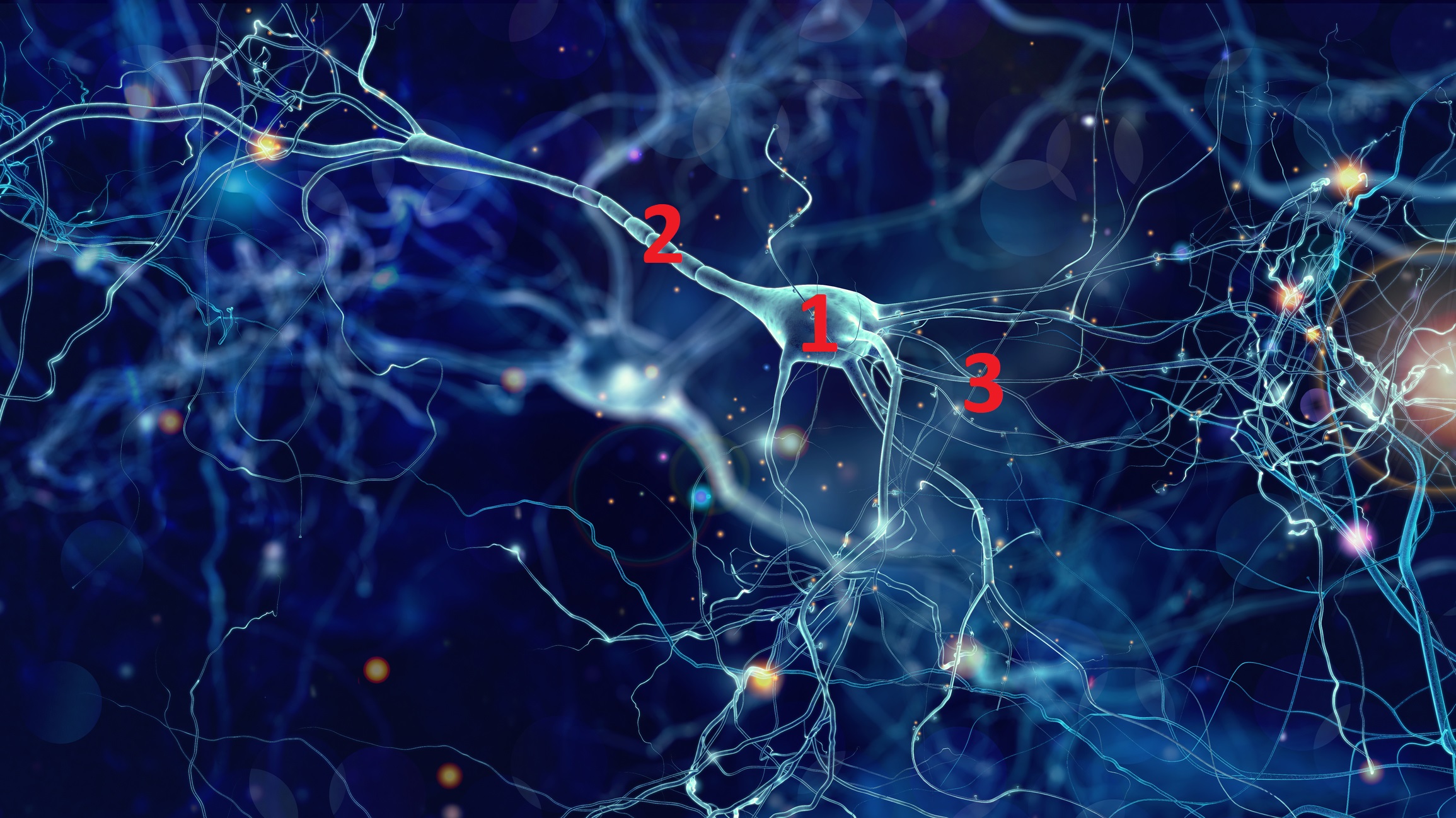
Neurons are made up of three parts.
A cell body, also called soma (from the Greek somâ meaning body): It is the “thinking head” of the neuron containing a nucleus and an “apparatus” (composed for example of mitochondria which provide the cell with energy) necessary to its proper functioning. It also provides most of the nutritional needs for keeping the neuron alive. The disruption of this apparatus leads to the death of the neuron; it is at the origin of neurological diseases such as Alzheimer’s disease or Parkinson’s disease which are qualified as neurodegenerative diseases.
An axon (from the Greek axôn meaning axis): it is a single arm which starts from the cell body and ramifies at its end. it is also called nerve fiber. Its length varies from a few millimeters, as in the case of small neurons in the brain, up to one meter in the case of axons that start from the spinal cord to innervate the feet.
Dendrites (from the Greek meaning dendron shaft): fine and short extensions forming a tree around the cell body. Most of the signals transmitted by neurons enter through dendrites, while other signals enter the cell body. Signals from neurons and projecting onto other neurons go through contact points called synapses. There is therefore no direct contact between neurons.
Thus, the neuron can receive information, store it and transmit it to other neurons.
The functioning of a neuron depends on its ability to communicate with its peers. This communication takes place using points of contact called synapses (from the Greek sun and aptein meaning respectively with and to join). A neuron has several thousand synapses located mainly between the axon of one cell and the dendrites of another cell.
During normal aging, synapses change morphology but remain relatively intact, while their number significantly decreases in the brains of people with Alzheimer’s disease.
Illustration of neurons with an soma (1), an axon (2) and dendrites (3).
The different types
There are different types of neurons depending on the size and shape of the soma, the density of the dendrites, as well as the length and branching of the axon.
Interneurons
Interneurons are found throughout the human body. Interneurons allow communication between sensory or motor neurons and the central nervous system.
Unlike the peripheral nervous system, the central nervous system – which includes the brain and the spinal cord – contains many interneurons. In the neocortex, which makes up about 80% of the human brain, 20% to 30% of neurons are interneurons.
Motor neurons
They have a cell body located in the brainstem, motor cortex, or spinal cord of the body. Its axon, or fiber, protrudes either on the spinal cord or outside the spinal cord in order to directly or even indirectly control the effector organs; in other words, the glands and the muscles.
A single motor neuron can innervate many muscle fibers.
Sensory neurons
They are nerve cells located in the nervous system and responsible for converting external stimuli from the body’s environment into internal electrical impulses.
This process is among the functions that include muscle contractions and even involuntary behaviors such as pain avoidance. These reflex circuits are usually found in the spinal cord in humans.
Also known as afferent neurons, sensory neurons convert a particular type of stimulus into action potentials through their receptors.
Information travels from the sensory nerve to the brain via the spinal cord. Stimuli can come from outside the body, including sound and light; or inside the body, including blood pressure or the sense of body position. Different types of sensory neurons have different receptors that respond to different types of stimuli.
The different types and functions include:
Taste : found in the taste receptors of the taste buds.
Odor : olfactory receptor neurons that are activated by odor molecules present in the air.
Vision : use of photoreceptor cells that convert light into electrical signals.
Auditory : responsible for converting pressure waves from air molecules or sound into signals that can then be interpreted by the brain.
Temperature : sensory receptors that react to varying temperatures.
Mechanoreceptors : These are sensory receptors that respond to mechanical forces, including distortion or pressure.
Do neurons have the same morphology?
No. Neurons, basic elements of the brain, have a very variable morphology. They are distinguished, among other things, by:
the shape of their cell body;
the organization and morphology of extensions (i.e. dendrites and their axons) emerging from the cell body.
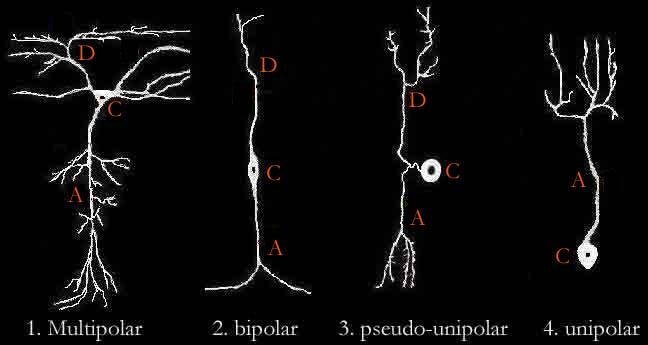
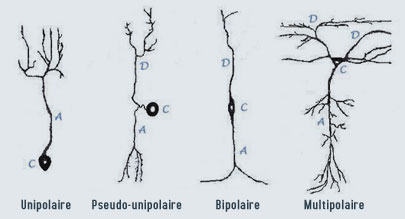
Here are schematically the four types of neurons found in the central nervous system (together making up the brain and spinal cord):
Unipolar neurons are found mostly in insects, with the cell body located outside the brain. These neurons have only one long extension (the axon) extending from the cell body (C).
Pseudo-unipolar neurons are sensory neurons located in the spinal ganglion. They pick up information from sensory receptors (e.g. pain receptors) through its dendrites and communicate it via its axon to the dorsal root of the spinal nerve to the spinal cord. The single dendrite (D) and the axon (A) are joined close to the cell body before they separate.
Bipolar neurons are rather rare sensory neurons specialized in the transmission of the senses (smell, sight, taste, hearing) and vestibular functions (balance, detection of movement). They are found in particular in the retina and the olfactory mucosa. The axon and the single dendrite are opposed to the cell body.
The multipolar neuron (4) is distinguished as well by the shape of its cellular body …… as by the shape of its axon or its dendrites. The multipolar neuron has a single axon and imposing dendrites (we speak of « dendritic tree »). Multipolar neurons constitute the majority of neurons in the brain.
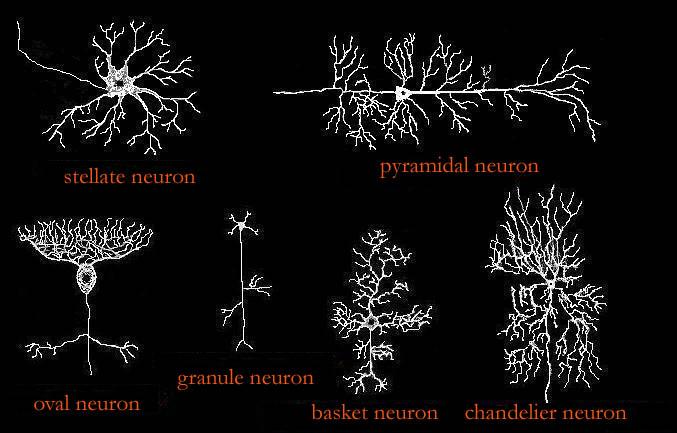
Different types of multipolar neurons
The axon of a neuron can be long (from a few centimeters to a few tens of centimeters): it is the type I Golgi neuron. It may, for example, be a pyramidal cell, the cell body of which, located in the cerebral cortex, may extend to the spinal cord.
The neuron can have a short axon (a few hundredths of a millimeter) that divides rapidly to give a complex arborization. This type of neuron remains within the limits of the structure in which it is found: it is the Golgi type II neuron. It can be, for example, a neural cell in a basket or in a star.
For some neurons, the axon and its collaterals present swellings called “spider veins” along their path. For other neurons, dendrites have irregular contours (called « dendritic spines »).
Multipolar neurons are, for example, motor neurons responsible for motor control from the cortex to the spinal cord or from the marrow to the muscles, but also interneurons which conduct impulses inside the central nervous system. Multipolar neurons make up the majority of neurons in the brain.
In summary, there are different types of neurons that come in very different forms. This polymorphism has an impact on the ability of the neuron to receive and process the information it receives from another neuron.
The multipolar neuron’s (1) morphology is diverse and is
distinguishable not only from the shape of the cell body, but also from the
shape of the axon or dendrites.
Are you looking for a way to improve your chances of winning big at the casino? With this guide, you’ll learn how to train your brain for peak performance when it comes to casino games such as Woo Casino slots. From mental concentration tips to strategies that maximize your chances of success, take a few minutes now to discover the best way to win in any casino game.
Study Strategies of the Game
Before playing any casino game, it’s important to understand all the rules of the game and study proven strategies from successful players. Knowing which moves may be a winner and understanding when it’s best to fold can give you a huge advantage in any setting. Play smart and maximize your chances for success. Make sure to do your due diligence researching effective strategies, so you can maximize your winnings within the casino environment.
Online casino withdrawal limits
Online casino withdrawal limits are in place to prevent users from withdrawing excessive amounts of money. These limits vary between different online casinos and will normally be set at a certain amount per day, week, or month. For example, a casino may have a withdrawal limit of $500 per day. By setting these limits, the casino can ensure that players keep their gambling behaviour in check and discourage unwise spending.
Set Affordable Limits and Stick to Them
Setting a budget is an important part of gambling. It’s critical to understand the difference between gaming and investing. Decide how much you’re willing to spend, and never bet more than that amount. This will help you focus on achievable winnings rather than impossible losses. It’s also wise to set short-term as well as long-term goals so that you have something to shoot for when you hit your target budget number.
Time management
Effective time management when playing at an online casino is important for a number of reasons. Keeping track of how long you are playing will help to ensure you stay within your budget and have more enjoyable experiences. This can be done by setting limits on the amount of time or money that you are willing to spend in each gaming session. Proper time management will also allow you to make the most out of your gaming experience by allowing you the opportunity to explore different aspects of the casino.
Take Regular Breaks from Gambling
Taking regular breaks from gambling is an important part of the training process. When playing casino games for an extended period of time, your brain can become over-stimulated and it can cause your performance to suffer. To avoid this, take a few minutes each hour to step away from the game and relax. This will allow you to reset your focus and come back more refreshed and ready to continue playing. Doing this also gives you a chance to evaluate how well you’re doing, so that you can adjust your strategy accordingly if needed.
Check Your Emotions at the Door
Emotions can be difficult to control when gambling and can ultimately lead to costly mistakes. Train your brain to dial down on the emotions by taking a few deep breaths before you begin playing, or stepping away from the game whenever your emotions start getting out of control. Remind yourself that it’s just a game, and try to remain focused on making decisions based on logic, rather than being influenced by emotional reactions.
Memory games sharpen your mind and slow down mental decline. Besides, these games also improve your focus, and you can be alert for longer. If you’re struggling with dementia, you should play memory games.
You can become more adept at recognizing patterns and remembering fine details by challenging memory games.
On top of all, playing memory games is a fun way to spend time and alleviate stress! In the following blog, we will discuss 6 reasons to play memory games. Let’s start with a better understanding.
Memory Games Improve Brain Function
Memory games keep your brain sharp. Regular engagement improves brain function and can delay age-related cognitive decline.
They can also help to sharpen concentration and increase problem-solving skills. These games range from simple card-matching games to more complex ones, such as Canadian online casinos, crosswords, or Sudoku puzzles. Playing whatever type of game you choose will keep your brain functioning at its best.
Boost Critical Thinking
Memory games boost critical thinking skills and improve memory. This is an enjoyable way to sharpen the minds of adults and children.
Regularly playing these games helps with short-term recall and strengthens overall cognitive abilities.
They involve remembering patterns or images, sorting cards, memorizing facts or words, and solving logic puzzles, among other activities that help strengthen recall capabilities.
Not only are they fun to play, but they also provide multiple benefits for brain development and learning potential. Regular playing of memory games leads to improved academic performance in math and reading comprehension. Besides, it can help decrease the chances of developing age-related illnesses like Alzheimer’s and dementia.
Enhance Visual Recognition
Memory games are good for visual recognition. They improve short-term memory and visual recognition skills.
They keep mentally sharp and reduce the risk of dementia and other cognitive decline in seniors. So, to improve your visual imagery, you should play memory games with high-tech visuals.
Improve Short Term Memory
Memory games are a fun way to increase your short-term memory. Playing memory games can help to improve recall, focus, concentration, and mental agility.
Many different types of memory games are available that use various techniques such as association, patterns, symbols, repetition, word games, and more to help you improve your memory.
They also provide an enjoyable way for people of all ages, such as real money casinos. Plus, it’s a great time with friends or family.
Memory games may Improve Decision Making
Memory games improve your decision-making skills. By playing memory games, you can boost your ability to focus and make quick decisions. This is because the game requires you to recall and match items quickly to win.
Practicing this type of activity helps sharpen your mental understanding, which can then be applied in other areas of life where making quick decisions is necessary.
Besides, they can help develop problem-solving skills as they require players to create strategies to win. These activities are useful for improving cognitive functions, making them a beneficial pastime for people of all ages.
Improve Your Focus
Memory games could be a perfect option if you want to sharpen your focus. They can strengthen your ability to concentrate, and you can pay attention for extended periods.
The more you play, the better your results will be! Regularly engaging in cognitive activities such as playing memory games helps protect against memory loss diseases later in life.
To summarize, if you want to learn life-changing lessons, you must play memory games. These can change your life and make you productive in every field of life.



{kind=link}