Vascular dementia is recognized as multiple infarct dementia resulting from successive strokes.
It was described at the end of the 19th century by doctors Binswanger and Alzheimer.
Vascular dementia includes heterogeneous categories of vascular diseases, excluding those caused by asphyxia, respiratory failure or carbon monoxide poisoning.
It varies depending on the location and type of lesions associated with it. In nearly 70% of cases, these lesions affect the small vessels and the white matter in the regions
below the cortex (eg the amygdala).
Most studies indicate that vascular dementia is the second leading cause of dementia after Alzheimer’s disease, accounting for between 10 out of 20% of cases.
The prevalence of the disease varies from 1.2 to 4.2% in people aged 65 and over.
These figures should be taken with caution because unlike Alzheimer’s disease, there is no consensual definition and valid diagnostic criteria for vascular dementia. In addition, brain imaging is generally not performed in population studies.
The differential diagnosis between Alzheimer’s disease and vascular dementia is sometimes difficult because, on the one hand, the latter is not always associated with a vascular event and, on the other hand, its clinical evolution is gradual as in Alzheimer’s disease.
The causes of vascular dementia
There are several forms of lesions that cause the different forms of vascular dementia. These diseases are divided according to the regions of the brain affected, their frequency, and the size of the arteries and vessels affected. There is no official classification of
vascular dementias, but they can be classified as follows, inspired by the classification proposed by the clinician Roman.
- Dementia caused by multiple and extensive cerebral infarctions (or strokes), affecting cortical and subcortical regions that play a role in cognitive functions. These infarctions are often accompanied by mini-lesions damaging the white matter. Although this form reflects the classic view of vascular dementia, it is not the most common.
Clinical signs: focal neurological signs, cognitive disorders such as aphasia, apraxia, agnosia.
Its evolutionary course describes either a sudden onset and a stepwise worsening (one-third of cases), or an insidious onset and gradual evolution (one-third of cases).
2. Dementia caused by single lacuna-sized brain infarctions affecting a specific cortical and subcortical region that plays an important functional role. Cortical regions affected are the medial temporal lobe, angular and cingulate gyrus, while
subcortical regions affected are the thalamus, caudate nucleus, internal capsule and anterior cerebral artery. These infarcts generally affect both hemispheres.
Clinical signs: memory disorders, executive function disorders, confusion, apathy, behavioral disorders.
3. Dementia caused by damage to small vessels (also called subcortical ischemic vascular dementia). These small vessels are either obstructed by atherosclerosis leading to the formation of several gaps, or narrowed (phenomenon of stenosis) leading to partial infarctions of the white matter . This dementia affects subcortical regions (as seen in Binswanger’s disease, rare CADASIL, multiple lacunae), or cortical and subcortical regions (arteriolosclerotic and hypertensive angiopathy, amyloid angiopathy). This form of dementia presents with mini-lesions or multiple white matter lacunae, located particularly in the frontal regions.
Clinical signs: psychomotor and balance disorders, urinary incontinence, cognitive disorders (executive functions and to a lesser extent memory) and behavior (mood). Balance disorders worsen as the disease progresses. Patients become increasingly apathetic, exhibit rapid and significant changes in mood (emotional lability), loss of attention, perseverations (stereotypical behavior of repeating the same word, performing the same movement, in response to various questions or tasks requested).
4. Dementia caused by hypoperfusion:
• Diffuse anoxic encephalopathy (anoxic: decrease in the amount of oxygen).
• Incomplete white matter infarction.
5. Hemorrhagic dementia, caused by subdural hematoma (hematoma of the meningeal spaces, between the arachnoid and the dura mater), subarachnoid hemorrhage, or venous thrombosis. MRI has identified chronic hemorrhagic lesions characterized by the presence of hemosiderin deposits (iron deposits impregnating the tissues).
Diagnostic criteria
There are at least eight diagnostic criteria for vascular dementia, reflecting the lack of consensus among the medical community.
The main ones are: Hachinski ischemic score, DSM-IV, NINDS-AIREN criteria, ICD 10, ADDTC criteria (State of California Alzheimer’s Disease Diagnostic and Treatment Center).
NINCDS–AIREN Criteria
These criteria divide the patient into three stages: probable, possible and definite vascular dementia.
The three criteria for probable vascular dementia:
- Presence of dementia characterized by impairment of episodic memory and at least two other cognitive domains: orientation, attention, language, visual and spatial abilities, executive functions, motor control and praxis. They are significant enough to interfere with activities of daily living.
Exclusion criteria: impaired consciousness, confusion, psychotic symptoms, severe aphasia, major sensorimotor disorder preventing neuropsychological assessment, other
brain diseases (such as Alzheimer’s disease). - Presence of cerebrovascular disease defined by focal neurological signs (hemiparesis, central facial paralysis, Babinski’s sign, sensory deficit, hemianopsia, dysarthria on neurological examination, and the presence of cerebrovascular disease demonstrated by brain imaging.
- A relationship between dementia and cerebrovascular disease manifested by the presence of at least one of the following three points:
- onset of dementia within 3 months of stroke
- sudden deterioration of cognitive functions;
- a fluctuating or stair-stepping course of cognitive impairment;
Elements supporting the diagnosis of vascular dementia:
- presence of an early gait disorder (walking with small steps);
- a history of instability or frequent unprovoked falls;
- urinary disorders unexplained by a urological condition;
- pseudobulbar palsy;
- personality or mood changes, abulia, depression, emotional lability, psychomotor retardation and executive function abnormalities.
The diagnosis of vascular dementia is questioned if the progressive deterioration of cognitive functions is not accompanied by vascular lesions (validated by scanner or MRI) or neurological signs.
The criteria for possible vascular dementia are:
- presence of dementia and neurological signs when no neuroimaging study is available or;
- no clear temporal relationship between dementia and stroke or;
- insidious onset and variable fluctuating course of cognitive deficits.
The criteria for definite vascular dementia are:
- a clinical history of probable vascular dementia;
- anatomical evidence of cerebrovascular disease (e.g. after autopsy);
- absence of neurofibrillary tangles and abnormally high amyloid plaques for age;
- the absence of other clinical or pathological signs capable of causing dementia.
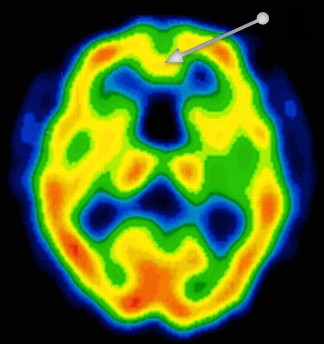
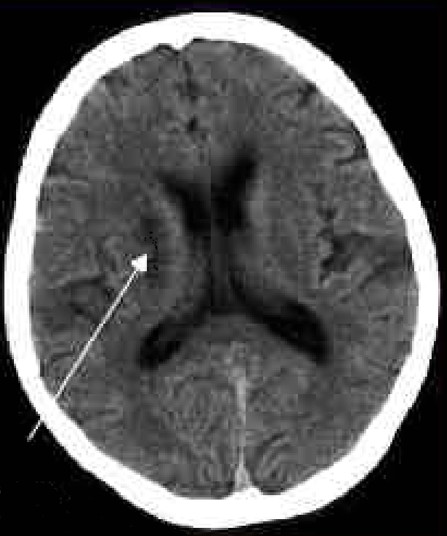
Magnetic resonance imaging of a brain of a person with vascular dementia. In the region of the frontal lobe (arrow), a decrease in cerebral blood flow significant of a severe lesion is observed. This decrease is characterized by a yellow color, while the red color reflects a normal flow. The lesion is characteristic of neuronal death leading to a decrease in oxygen consumption by the neurons.
Brain imaging techniques
The different cerebral imaging techniques make it possible to determine the presence of significant anomalies responsible for the different types of vascular dementia. They complete the diagnostic criteria.
Forms of brain imaging are:
- Magnetic resonance imaging, the most widely used method to assess cerebrovascular pathology.
- Functional magnetic resonance imaging. It assesses how the functions of different brain regions are reorganized following vascular dementia.
- Positron emission tomography (PET) imaging. It is a technique that measures the metabolic activity of brain regions by injecting the radioactive tracer called 18-fluorodeoxy-D-glucose. In vascular dementia, decreased metabolism is seen in the association cortex (as in Alzheimer’s disease), primary cortices, basal ganglia, thalamus, and cerebellum.
- Single photon emission tomography (SPECT). Unlike PET, SPECT only detects a single photon (while PET detects two), which decreases the spatial resolution of the images. However, it is a much more accessible method, because on the one hand the radiotracers are more available (they do not require emitting positrons) and on the other hand the imaging system is simpler.
- Despite the usefulness of these techniques, functional neuroimaging cannot distinguish the lesions associated with Alzheimer’s disease from those observed in vascular dementia.
Blood tests
Doctors may need to order lab tests to check for health indicators that aren’t apparent in a person’s recent medical history. This may include tests to check their cholesterol or blood sugar levels.
They may also order additional tests to help rule out other issues that may be causing similar symptoms, such as vitamin deficiencies, anemia, and thyroid disorders.
The signs and symptoms
Cognitive functions
Vascular dementia is characterized by:
- early impairment of executive functions (planning, abstract thoughts),
- attention deficit, decreased verbal fluency (semantic memory disorder) and
- deterioration of visual-spatial functions.
These 3 types of cognitive disorders are more marked than in Alzheimer’s disease.
On the other hand, episodic memory is less affected in vascular dementia than in Alzheimer’s disease.
There is a correlation between the location of brain damage and the type of cognitive impairment patients suffer from.
With regard to vascular accidents of small vessels, characterized by lesional damage limited to the subcortical regions, cognitive deficits are quite frequently limited to impaired executive functions (flexibility, inhibition, working memory). Memory damage, characterized by a deficit in retrieving a memory, makes it possible to differentiate these disorders from those observed in Alzheimer’s disease.
With regard to vascular accidents of the large vessels (lesional damage affecting both the cortical and subcortical regions), establishing a differential diagnosis proves to be much more difficult. In general, episodic memory (measured by the word recall test) is better preserved in vascular dementia than in Alzheimer’s disease. Degradation of working memory (characterized for example by the ability to repeat a series of numbers) is also very common in this type of lesion.
Some clinicians suggest removing the notion of memory decline as a diagnostic criterion.
Functional autonomy
Functional decline in basic activities of daily living appears to be identical in vascular dementia and Alzheimer’s disease, whereas decline in instrumental activities of daily living (eg managing money) appears slower in vascular dementia.
Behaviour
Behavioral disorders are generally similar to those observed in Alzheimer’s disease. Depressive symptoms, emotional behavioral disturbances, and apathy appear to be more common in vascular dementia than in Alzheimer’s disease.
Risk factors for vascular dementia
Risk factors for vascular dementia can include smoking, obesity, and high blood pressure.
The risk of vascular dementia tends to increase as a person ages. The National Heart, Lung, and Blood Institute states that the disease affects nearly a third of people over the age of 70.
Additionally, a number of other factors and conditions can increase the risk of damaged blood vessels and vascular dementia, including:
- smoking
- obesity
- abnormal heart rhythms
- high cholesterol
- high blood pressure
- atherosclerosis
- diabetes
- a history of heart attack or stroke
Evaluation of vascular dementia
Cognitive functions
The Alzheimer’s Disease Assessment Scale (ADAS-cog), a scale used in Alzheimer’s disease, explores numerous functions (memory, comprehension, temporal-spatial orientation and spontaneous language) altered in vascular dementia. The Trail Making B (tracing test) or the EXIT-25 are used in addition to assess executive functions.
Functional autonomy
Functional decline in basic activities of daily living appears to be identical in vascular dementia and Alzheimer’s disease, whereas decline in instrumental activities of daily living appears to be slower in vascular dementia.
The Disability Assessment in Dementia Scale (DAD) and the Interview for Deterioration in Daily Living Activities in Dementia (IDDD) are functional scales taking into account the consequences of executive function disorders in dementia. These scales make it possible to determine whether the functional incapacity originates from a cognitive deficit (for example difficulty handling money) or a motor deficit (difficulty walking).
Behaviour
The Neuropsychiatric Inventory is, together with the Behave-AD, an appropriate rating scale.
Vascular dementia and Alzheimer’s disease: the differences
There are many differences between vascular dementia and Alzheimer’s disease: prevalence, causes, clinical signs.
Prevalence
Alzheimer ‘s disease is by far the most common type of dementia. It accounts for about two-thirds of dementia cases.
It is estimated that vascular dementia accounts for 10% to 20% of dementia cases.
About 50% of older people with dementia (especially Alzheimer’s type) show signs of vascular dementia. We then speak of mixed dementia if the vascular dementia is associated with dementia of the Alzheimer type.
The causes
Vascular dementia is often caused by a specific acute event, such as a stroke or a transient ischemic attack in which blood flow to the brain has been interrupted. It can also develop more gradually over time as a result of slow blood flow.
The causes of Alzheimer’s disease are not understood, although it is known to be characterized by a buildup of proteins in the brain called amyloid and tau. There seem to be many components, such as genetics, lifestyle, and other environmental factors.
Diagnostic criteria
| Alzheimer’s disease | Vascular dementia |
| 1. Presence of dementia 2. Onset between 40 and 90 years of age 3. Deficits in at least 2 cognitive domains 4. Progression of deficits lasting longer than 6 months 5. Unimpaired state of consciousness 6. No other diagnosis made . | 1. Presence of dementia 2a. Focal neurological signs 2b. Vascular lesions observed by cerebral imaging 3. Association of 1 and 2 with either: – the existence in the previous 3 months of a cerebrovascular accident or; – sudden cognitive deterioration. |
Clinical profiles
The differences between vascular dementia and Alzheimer’s disease also concern the clinical signs.
In the case of vascular dementia: cognitive abilities often seem to decrease sharply in relation to an event such as a stroke or transient ischemic attack (TIA), then remain stable for a period of time.
In the case of Alzheimer’s disease, cognitive functions gradually decline over time. There are usually no sudden, large changes from one day to the next.
Treatments
There is currently no cure for vascular dementia because there is no way to reverse brain damage. However, it may be possible to slow or sometimes stop the progression of the disease by controlling certain risk factors, for example.
Antihypertensives
Antihypertensives are recommended in hypertensive individuals to reduce the risk of cardiovascular disease. However, there is no consensus regarding the effectiveness of these drugs in reducing the risk of dementia. A study published in 2013 reports this fact, but points out that calcium channel blockers (e.g. lercanidipine, nitrendipine) seem more effective. Some clinicians point out that lowering blood pressure can have deleterious effects in people with cerebrovascular disease. Further studies are needed to determine optimal blood pressure in individuals at risk for vascular dementia.
Antidiabetics
Blood sugar management is recommended in the prevention of diabetes-related complications. The studies that have analyzed the association between diabetes and dementia are not of good enough quality to draw a conclusion.
Statins
Taking statices reduces the risk of dementia in people with high cholesterol. However, if we look at the different forms of dementia, there is no association between taking statins and the risk of vascular dementia.
Antiplatelets
To date, there is no evidence that regular aspirin consumption reduces the risk of developing vascular dementia and slows its progression.
The results of a phase III clinical trial have shown that the combination of anticoagulant drugs (clopidogrel (Plavix) and aspirin) – decreases the risk of recurrence by about a third in patients who have suffered a transient ischemic attack . This decrease is compared to the group of patients who received only aspirin. 8.2% of patients taking both drugs relapsed within three months compared to 11.7% in those taking only aspirin (Source: Clopidogrel with Aspirin in Acute Minor Stroke or Transient Ischemic Attack. New England Journal of Medicine, 2013).
Vitamin B
B vitamins are prescribed to lower blood homocysteine, new highs of which are a cardiovascular risk factor. Several studies have shown the effectiveness of a combination of vitamins B2, B6 and B12 in elderly people suffering from vascular diseases. However, although homocysteine levels were reduced, this treatment was not accompanied by an improvement in cognition.
Lifestyle
It is recognized that the adoption of a healthier lifestyle (stopping smoking, moderate alcohol consumption, physical activity and healthy eating) is associated with better cognitive performance towards old age. Observational studies indicate that intellectual activity (eg bridge) is associated with a reduced risk of mixed and vascular dementia, as well as cognitive impairment of vascular origin.
In addition, such a reduction in risk is observed in those who practice physical activity frequently, compared to inactive people.
Acetylcholinesterase inhibitors
Lack of acetylcholine – the memory neurotransmitter – in the brain is not only seen in Alzheimer’s disease, but also in vascular dementia.
The three acetylcholinesterase inhibitors, aimed at increasing the level of this neurotransmitter in the brain, are also prescribed in the treatment of vascular dementia.
Calcium channel blockers
A meta-analysis concludes that nimodipine (90 mg/day) improves some aspects of cognition, but has no positive effects on activities of daily living. Clinical studies over longer periods (one to two years) are needed to confirm these results. No beneficial effects have been reported with nicardipine and cyclandelate.
Clinical case
A 75-year-old patient is undergoing abdominal surgery. Following this operation, she was again hospitalized for incoherent speech and occasional hallucinations. He was diagnosed with postoperative confusion, cognitive impairment (his mini-mental state exam score was 16/30), and mood disorders.
The doctor prescribed him an antidepressant and an antipsychotic. She then returned to her nursing home. A year later, the patient presented with Parkinsonian-like symptoms (tremor, rigidity) which, together with a cognitive deficit, suggested dementia with Lewy bodies. The doctor prescribed Aricept (a drug used in the treatment of Alzheimer’s disease) and piripedil.
Four years later, the patient entered a long-term care center because she frequently fell due to severe limb rigidity and psychomotor retardation. The treatment with the neuroleptic (known to cause motor disorders) is then stopped. His cognitive performance stabilized with an MMSE score identical to that obtained four years previously. However, she suffers from temporal disorientation, moderate executive function disorders, difficulty memorizing information and retrieving it.
The medical staff suggested the existence of subcortical frontal dementia. However, the neuroimaging examination (magnetic resonance imaging) reveals the presence of ischemic-type vascular lesions as well as diffuse leucoaraiosis.
Diagnosis of this clinical case: the patient probably suffers from vascular dementia.
1 Piripédil (trade name: Trivastal®, France): medicinal product used in particular in the adjunctive treatment of chronic pathological cognitive and neurosensory deficit in the elderly (excluding Alzheimer’s disease and other dementias).