La neuroinflammation
Commentaires fermés sur La neuroinflammationLa neuroinflammation est une réaction inflammatoire qui se déroule dans le cerveau et au cours de laquelle s’expriment des molécules appelées cytokines.
Les tissus réagissent en réponse à une infection ou à la présence d’un corps étranger : cette réaction inflammatoire se caractérise par des rougeurs ou une lésion fonctionnelle.
Les acteurs participant à ces phénomènes sont les globules blancs (appelés leucocytes) produits par la moelle osseuse et présents dans le sang.
Le nombre des leukocytes augmente lors de l’inflammation.
Il existe trois grandes classes de globules blancs : les lymphocytes, les granulocytes et les monocytes.
- Les lymphocytes participent à la réaction immunitaire en produisant des anticorps qui vont aider à détruire l’agent pathogène (par ex. une bactérie).
- Les granulocytes qui sont des globules blancs qualifiés de « non spécifiques » à un antigène.
- Les monocytes sont des cellules du sang qui phagocytent (du grec phagos, manger; la phagocytose a été mise en évidence au début du XXème siècle par le biologiste russe Elie Metchnikoff), c’est-à-dire qu’ils avalent et digèrent les débris cellulaires et les particules vivantes (par ex. des microbes).
Il existe un autre type de cellules « dévoreuses » ayant les mêmes propriétés que les monocytes: ce sont les macrophages (du grec makros, grand). Alors que les monocytes se situent spécifiquement dans le sang, les macrophages sont localisés dans les tissus.
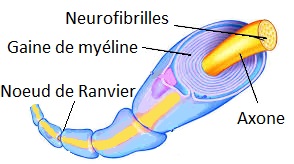
Il existe ainsi des macrophages dans le cerveau qui portent le nom de cellules microgliales: elles forment avec les astrocytes et les oligodendrocytes les cellules gliales (lire l’article sur le (article sur le fonctionnement du cerveau).
Le cerveau peut-il être la cible d’une inflammation ?
On croyait jusqu’à récemment que le cerveau bénéficiait -contrairement aux autres organes- d’un privilège immunitaire et qu’il échappait largement à la surveillance immunitaire. Il n’en est rien.
La cellule microgliale joue à ce titre un rôle évidemment central puisque c’est la cellule qui phagocyte les éléments étrangers. Mais elle peut également se retourner contre les cellules voisines, c’est-à-dire les neurones, notamment lors de troubles neurologiques. C’est en quelque sorte Dr. Jekyll et Mr. Hyde.
Ainsi la maladie d’Alzheimer s’accompagne d’une activation des cellules microgliales. Cette réaction provoque une réaction inflammatoire appelée neuroinflammation, au cours de laquelle s’exprime une bonne centaine de molécules différentes et que l’on appelle cytokines.
Les cytokines
La caractéristique d’une réaction immunitaire et d’une neuroinflammation est la production de cytokines (du grec kutos, cellule, et kinéo, stimuler), messagers chimiques permettant aux cellules de communiquer entre elles.
Elles sont donc libérées par les cellules gliales lorsqu’un agent infectieux ou toxique attaque l’organisme.
Les cytokines vont ainsi induire, contrôler ou inhiber l’intensité et la durée de la réponse immunitaire. Lorsque les cytokines sont sécrétées par les cellules, elles agissent:
- en circulant dans le sang (c’est le mode endocrine, du grec endon, au-dedans; ekkrinein, excréter),
- en agissant sur les cellules qui les sécrètent elles-mêmes (c’est le mode autocrine, du grec auto, en soi) ou
- en agissant sur les cellules voisines (c’est la mode paracrine, du grec para, à côté de).
Elles sont impliquées dans un grand nombre de fonctions, en particulier dans la résistance aux agents infectieux ou toxiques. Elles englobent donc plusieurs domaines d’application : cancérologie, hématologie, immunologie, infectiologie et neurologie. Il existe une quarantaine de cytokines identifiées à ce jour, regroupées en familles. Celles jouant un rôle dans les troubles cérébraux sont :
– Les interleukines (IL) telles que l’interleukine 1 (IL-1).
– Le transforming growth factor-ß.
– Le facteur de nécrose tumorale (ou TNF-alpha pour tumor necrosis factor-alpha).
De nombreuses études ont montré que de nombreuses agressions au cerveau venant de traumatismes crâniens, d’accidents vasculaires cérébraux, d’infections ou de certaines maladies mentales (schizophrénie, maladie d’Alzheimer) sont associées à de fortes concentrations de cytokines (par exemple IL-1 ou TNF-alpha).
Ce phénomène de surproduction de cytokines dans le cerveau s’appelle la neuroinflamation.
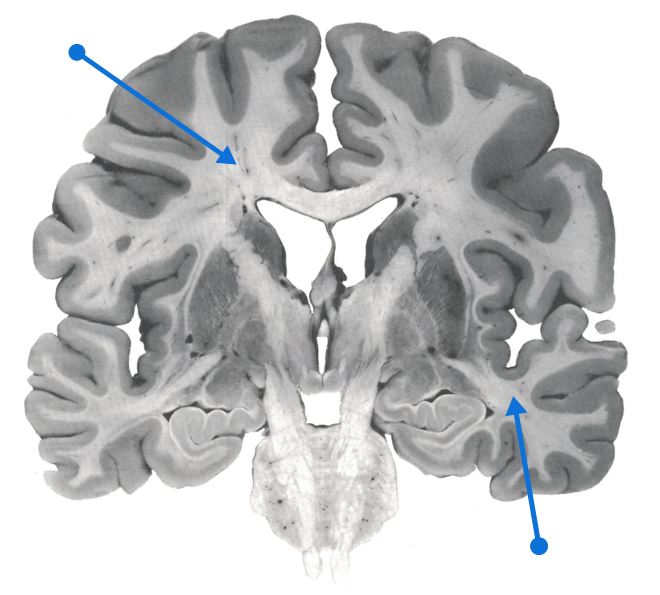
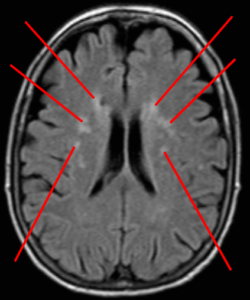
La neuroinflammation est impliquée dans la maladie d’Alzheimer
La neuroinflammation se caractérise donc par une libération accrue de certaines cytokines dans le cerveau de patients atteints de la maladie d’Alzheimer (MA). Une de ces cytokines serait particulièrement impliquée dans la MA: la TNF-alpha. En effet :
– Les niveaux de TNF-alpha sont 25 fois plus élevés dans le liquide céphalorachidien (liquide dans lequel baigne le cerveau) des patients MA que chez les personnes saines; de plus les patients souffrant de déclin cognitif léger et ayant des niveaux élevés de TNF-alpha ont un risque accru de développer une MA.
– Des polymorphismes génétiques* associés à une augmentation de la production de TNF-alpha ont été observés chez certaines populations ayant un risque accru de développer une MA.
* Polymorphismes génétiques : un gène a deux copies appelées allèles. Ces allèles peuvent exister sous différentes formes dans une population : c’est le polymorphisme. Cette différence d’expression n’engendre pas une maladie mais peut augmenter le risque de la développer.
– Selon une étude épidémiologique, une production de TNF-alpha par des cellules sanguines (macrophages, mastocytes) est associée à une augmentation du risque de développer une MA.
– Les études réalisées chez l’animal renforcent l’hypothèse d’un rôle de la TNF-alpha dans le dysfonctionnement des synapses (zones de contact entre les neurones) lors du vieillissement pathologique; en particulier lorsque les synapses sont exposées à l’amyloïde, protéine jouant un rôle inhibiteur dans la mémoire et dans la mort neuronale dans la MA.
Il a également été montré que le TNF-alpha et l’amyloïde rentrent dans un cercle vicieux dans lequel l’amyloide stimule les cellules microgliales, ce qui excite neurones et cellules gliales, qui fabriquent d`avantage de l’amyloïde, et ainsi de suite.
TNF-alpha et la maladie d’Alzheimer
L’excès de TNF-alpha produite par les macrophages va provoquer une réaction inflammatoire excessive qui va endommager les articulations et provoquer des rhumatismes inflammatoires telle que la polyarthrite rhumatoïde. Des molécules capables de bloquer l’action des TNF-alpha ont déjà été développées dans le traitement de cette maladie. Ces molécules sont : étanercept, infliximab et adalimumab. En se basant sur ces résultants, la communauté médicale s’est proposé de tester l’une de ces molécules chez des patients Alzheimer.


{kind=link}