Binswanger’s disease, also called subcortical vascular dementia, is a type of dementia caused by microscopic damage to the deep layers of white matter in the brain.
The damage is the result of thickening and narrowing (atherosclerosis) of the arteries that supply the subcortical areas of the brain.
Atherosclerosis usually begins in the late 40s and increases in severity with age. As the arteries become narrower and narrower, the blood supplied by these arteries decreases and the brain tissue dies.
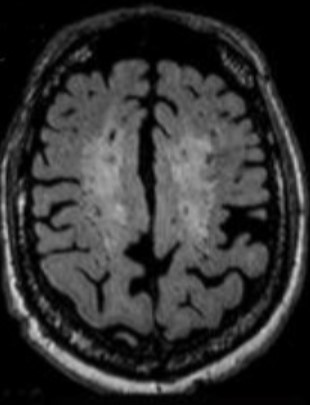
A characteristic pattern of damaged brain tissue in Binswanger’s disease can be seen with modern brain imaging techniques such as computed tomography or magnetic resonance imaging (MRI).
Binswanger’s disease results in white matter lesions in subcortical regions
Cerebral small vessel disease include Binswanger’s disease,
Cerebral small vessel disease (CSVD) refers to a constellation of various disorders relating to the vascular network in the brain, particularly concerning narrow capillaries, arterioles and venules. The advanced age of this vascular web as well as oxidation processes contribute to its degeneration and pathology. This medical condition can involve Binswanger’s Disease, leukoaraiosis, cerebral microbleeds (CMBs) or lacunar strokes; all representing particular forms at the different classifications of CSVD.
Symptoms
The most characteristic feature of Binswanger’s disease is psychomotor slowness – an increase in the time it takes, for example, for the fingers to transcribe thought from letter to letter on a piece of paper.
Other symptoms include forgetfulness (but not as severe as memory loss in Alzheimer’s disease), speech changes, unsteady gait, frequent falls, personality or mood changes (very probably in the form of apathy, irritability and depression), and urinary symptoms that are not caused by urological disease.
Brain imaging, which reveals the characteristic brain lesions of Binswanger disease, is essential for a positive diagnosis.
Treatment of Binswanger’s disease
There is no specific treatment. People with depression or anxiety may need antidepressant medication. Atypical antipsychotic drugs may be helpful in individuals with agitation and disruptive behavior.
Recent clinical trials with the drug memantine have shown improved cognition and stabilization of functioning and overall behavior.
Successful management of hypertension and diabetes can slow the progression of atherosclerosis, and subsequently slow the progression of Binswanger’s disease. Because there is no cure, the best treatment is preventive, controlling risk factors such as high blood pressure, diabetes, and smoking.
Binswanger’s disease is a progressive disease; there is no remedy. Changes can be sudden or gradual, then progress in stages. It can often coexist with Alzheimer’s disease. Behaviors that slow the progression of high blood pressure, diabetes, and atherosclerosis — such as eating healthy and maintaining healthy sleep/wake schedules, exercising, and not smoking or drinking too much alcohol — can also slow the progression of the disease.
Hypertension not only increases the risk of cardiovascular disease, but also that of Alzheimer’s disease.
Only half of individuals with hypertension are able to control their blood pressure, for various reasons: disease underestimated by the attending physician, poor medication intake by the patient, ineffective medication…
High blood pressure diagnosed between the ages of 35 and 64 increases the risk of Alzheimer’s disease by 61%, for various reasons:
it would promote the appearance of amyloid plaques which destroy neurons;
it would facilitate the narrowing of the small cerebral arteries which end up clogging, or even breaking, which leads to a mini-stroke.
On a global scale, taking into account the prevalence of arterial hypertension, its attributable risk in Alzheimer’s is 6.8%. Reducing the prevalence of arterial hypertension by 25% would reduce the number of Alzheimer’s patients by 100,000 in France.
In addition to antihypertensives, it is strongly advised to have a healthy lifestyle, for example by increasing physical activity.
In 2013, a study of autopsies of 774 men treated with a beta-blocker antihypertensive indicated that there were fewer cases of micro-brain lesions, cerebral atrophy, and lesions characteristic of Alzheimer’s disease. Alzheimer’s, compared to those who were not treated. Source: American Academy of Neurology meeting.
In summary, hypertension, or high blood pressure, is often linked to an increased risk of developing dementia, both of the vascular and Alzheimer’s types. It remains uncertain that hypertension is related to the aggregation of lesions higher plaques and tangles) of Alzheimer’s’ disease. A history of hypertension is believed to correlate with cerebrovascular changes that could potentially lead to dementia; however, the actual cause of this connection has yet to be determined. Midlife hypertension appears to be a particularly strong risk factor for late-life dementia whereas in later life, both low and high blood pressure readings can indicate an elevated risk.
An overview of Alzheimer’s disease: what are the risk and protective factors, signs and symptoms, diagnosis, assessment, causes and screening.
SUMMARY
The number of cases increases with age
Factors that increase the risk
Protective factors
Signs and symptoms
The signs that should worry us?
Diagnostic
Assessment
Etiology
Screening
Alzheimer’s disease is the most common dementia with 60% of dementia cases.
95% of cases are sporadic, affecting individuals in an isolated and irregular manner at a late age (over 65).
Hereditary forms (which are characterized by the transmission of ‘bad genes’) represent only about 5% of total cases. The genes involved in the family forms are the presenilin 1 and 2 genes (PSEN), leading to the onset of the disease in middle age (around 30 to 40 years depending on the mutated gene). The mutation being dominant, and since each parent transmits an allele (variant of the gene), a child is 50% likely to develop the disease.
There are also genetic predispositions caused by the mutation of certain genes, in particular the apolipoprotein E gene (APP) which increases the risk of developing the disease. The mutation is not dominant.
Some cases of early-onset Alzheimer’s disease are caused by genetic mutations that can be passed from parent to child. Researchers have found that this form can result from mutations in the APP and PSEN genes.
The number of Alzheimer’s disease cases increases with age
Five percent (5%) of people aged 65 and over are affected by the disease (8% suffer from dementia) in industrialized countries. The prevalence rate (total number of cases) increases exponentially with age, approximately doubling every 5 years. Fifteen percent of patients are under 75 years old. According to a report published in 2012 by the World Health Organization, Alzheimer’s disease affects from the age of 65 2.3% of men and 3% of women and affects 33% of men over 90 and 48. % of women of the same age. The table below summarizes the prevalence rate by age group and according to sex, which demonstrates that age is therefore the main risk factor and that women are more affected than men.
The tables below summarize incidence (number of new cases) and prevalence by age and gender.
Age
Prevalence rate
Impact
Men
65-69 years old
1
0.6
70-74 years old
3
1.5
75-79 years old
6
1.8
80-84 years old
12
6.3
>85 years old
20
8.8
Women
65-69 years old
1
0.7
70-74 years old
3
2.3
75-79 years old
6
4.3
80-84 years old
14
8.4
>85 years old
31
14.2
Sources: EUROMED, Paquid (France) The table below summarizes the incidence (number of new cases) according to age and sex.
Factors that increase the risk of Alzheimer’s disease
Age (main risk factor).
The low level of study.
The female gender.
Family history.
History of head trauma.
Depression.
Diabetes.
Untreated hypertension.
Genetic factors: in the sporadic forms of Alzheimer’s disease, a susceptibility factor has been demonstrated (the Epsilon 4 form of apolipoprotein E).
Toxic substances (controversial hypothesis at present).
Protective factors
Chronic use of nonsteroidal anti-inflammatory drugs. (hypothesis to be confirmed)
A healthy diet (Mediterranean diet).
Physical activity.
Cognitive activity.
Studies show that physically active people are less likely to experience a decline in mental function, and have a reduced risk of developing Alzheimer’s disease.
The multiplicity of these factors (probably interdependent) would explain why this disease presents itself under very diverse aspects and affects people unequally: thus it can affect a person aged 40 or 80 and its average duration after diagnosis varies from 5 to 8 years.
The signs and symptoms
People with Alzheimer’s disease often have difficulty remembering recent events, which interferes with their daily activities. This memory loss is often due to damage in a part of the brain called the hippocampus, which plays a critical role in day-to-day memory.
The stages of Alzheimer’s disease
There are different stages of Alzheimer’s disease depending on the severity of the symptoms:
Moderate stage
The disease is characterized by the insidious appearance of memory disorders (often denied by the patient) which evolve very gradually. These disorders may be accompanied by depression and/or anxiety. Memory problems gradually worsen, and other cognitive functions (e.g. planning, calculation) begin to be affected, leading to a (partial) inability to carry out certain activities of daily living (phoning, taking the bus, managing one’s budget).
Moderate to severe stage
The patient suffers from the advanced stage of anosognosia (he is no longer aware of his disorders), is disoriented in space and time. He has trouble communicating with those around him because of language, gnosis, praxis and attention disorders. The loss of autonomy now affects the basic activities of daily life (dressing, personal hygiene, moving around, toilets). Behavioral disturbances can occur at this stage and include agitation, hallucinations, aggressiveness towards those around them, delusional manifestations, sleep disturbances, apathy, ambulation, vocalization and stereotyped behaviors.
Severe stage
The patient has completely lost his autonomy. He eats less and less, weakens, facilitating the appearance of other mental disorders such as confusion, depression or slip syndrome (the patient lets himself die by refusing to eat). Other complications appear: falls with fractures, bedsores… The death of the patient occurs between 5 and 10 after the date of the first symptoms. The profile of clinical manifestations is given as an indication, as they are heterogeneous. In some patients, the symptoms start suddenly, while in others, the diagnosis of dementia can be made, for example, following a surgical operation (an operation sometimes causes mental confusion in an elderly person.
Diagnostic
in 1984, a group of researchers from NINCDS-ADRDA (National Institute of Neurological and Communicative Disorders and Stroke and Alzheimer’s Disease and Related Disorders Association) established diagnostic criteria. There are three diagnostic levels: possible (pre-mortem diagnosis), probable (pre-mortem diagnosis) and definitive (post-mortem diagnosis after biopsy).
These criteria are:
– Cognitive disorders (memory, language, judgment, reasoning, etc.) generally accompanied by behavioral and psychological disorders (agitation, depression, aggressiveness, wandering, insomnia, etc.) that can affect activities of daily living.
The symptoms of dementia have two main characteristics:
Symptoms appear in adulthood (mental retardation is not one of them).
The symptoms are in most cases progressive and irreversible (confusional and depressive states of the elderly are not included).
In 2010, the American Institutes of Health (National Institute of Health) adopted new diagnostic criteria for Alzheimer’s disease. They now take into account the breakthroughs made in neuroscience that have allowed a better understanding of the disease.
While the clinical criteria used since then described the last stage of disease progression (when symptoms of dementia had already manifested), the new guidelines consider all known stages of disease development, which progresses gradually and can cause brain changes over a decade before it becomes apparent.
The new criteria include three phases:
1. The first so-called preclinical phase. She describes changes in the brain, including the formation and accumulation of senile plaques made up of beta-amyloid aggregates. These plaques would be responsible for the death of neurons. The use of brain neuroimaging techniques and biomarkers* is now helping to determine if changes in the brain are warning signs of disease.
2. The second phase. It corresponds to episodes of memory loss that are sufficiently obvious to be measured and noted by those around them. On the other hand, they are not pronounced enough to cause the loss of autonomy.
3. The third and final phase. This is the phase of dementia currently described by the medical community.
* Neurologists are increasingly using biomarkers to observe the evolution of pathology. However, they cannot be routinely used to make a clinical diagnosis.
Complementary examinations (in particular neuroimaging examinations) do not contribute to the diagnosis of Alzheimer’s disease. They most often indicate enlargement of the cerebral ventricles and widening of the cortical sulci, reflecting neuronal loss.
However, this aspect can be observed in healthy elderly people, as well as in patients suffering from other forms of dementia. However, hippocampal atrophy is considered specific for Alzheimer’s disease, and may aid in diagnosis.
According to the American psychiatric manual DSM-IV, the patient must fulfill criteria encompassing the following symptoms:
A. Appearance of multiple cognitive deficits as evidenced by both:
1. memory impairment;
2. one or more of the following cognitive disturbances:
Aphasia (language disturbance);
apraxia (impaired ability to perform an activity despite intact motor functions);
agnosia (inability to recognize objects despite intact sensory functions);
disturbances of executive functions (making plans, organizing in time, having an abstract thought).
B. Cognitive deficits in criteria A1 and A2 represent a significant decline from previous level of functioning.
C. The course is characterized by a gradual onset and continuous cognitive decline.
D. The cognitive deficits of criteria A1 and A2 are not due to:
other conditions of the central nervous system (eg cerebrovascular disease, Parkinson’s disease, brain tumour);
general conditions that can lead to dementia (eg hypothyroidism, vitamin B12 deficiency, HIV infection, etc.) substance-induced conditions.
E. Deficits do not occur exclusively during delirium.
F. The disturbance is not better accounted for by a disorder such as depression or schizophrenia.
Assessment
The evaluation of Alzheimer’s disease includes an interview with the patient and a family member, neurological tests, clinical examinations and neuroimaging.
Neuroimaging techniques can confirm or invalidate the diagnosis.
These techniques are:
• The electroencephalogram (EEG): this examination aims to see the electrical activity of the brain.
• Single photon emission tomography (SPECT): this assesses blood flow and the volume of cerebral regions.
• Positron emission tomography (PET): this studies the activity of brain regions. For example, patients with Alzheimer’s disease have reduced activity in the temporal and parietal lobes.
• Computed tomography: this measures the thickness of the regions of the brain affected in Alzheimer’s disease.
• Magnetic resonance imaging ( MRI): this visualizes changes in the structure of the brain.
• Functional magnetic resonance imaging (fMRI): this measures the functional activity of brain regions.
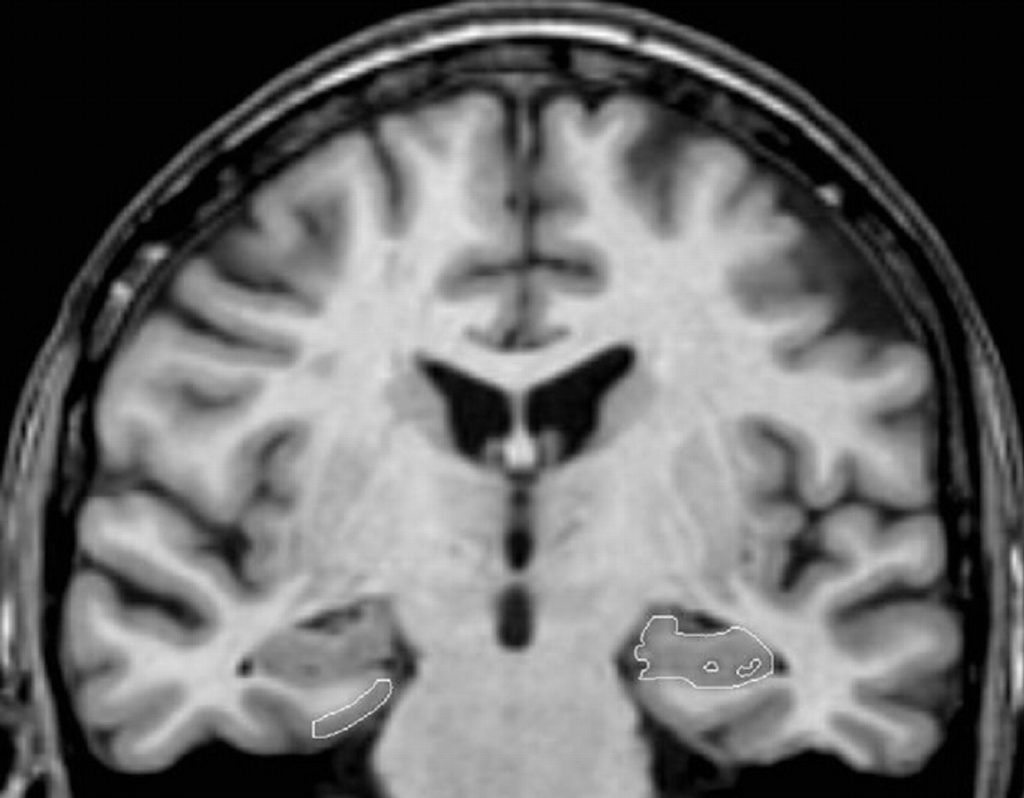
Image of a cross-section of the brain of a patient with Alzheimer’s disease obtained by magnetic resonance imaging
Blood and urine and cerebrospinal fluid tests to reveal vitamin deficiency, hormonal dysfunction, the presence of toxic agents or molecules involved in Alzheimer’s disease (e.g. amyloid protein)
Medical history ( e.g. history of head trauma, use of substances that may alter mental status).
Neuropsychological tests: the neuropsychological assessment contributes to the diagnosis in mild to moderate forms, by emphasizing the importance of memory disorders in relation to the deficit of other cognitive functions.
The MMSE is the most frequently used test because it quickly gives valuable information about short-term memory and other cognitive functions.
The other tests are the Clinical dementia Rating Scale, the ADAS scale (Alzheimer’s Disease Assessment Scale), the clock test, the free and cued recall test according to the procedure of Grober and Buschke and the five-word test.
Alzheimer’s disease, in the early stages, can be diagnosed through two neuropsychological examinations carried out +/- 6 months apart.
This delay will inform the doctor about the progressive nature of the disease (the evolution confirms the initial diagnosis).
Behavioral tests ( CERAD Behavior Rating Scale for Dementia, the neuropsychiatric inventory) are used to assess the frequency and severity of behavioral disorders.
Functional tests assess the degree of autonomy of patients, for example instrumental activities of daily living.
The causes
The causes of the disease remain unknown, but it is already strongly suspected that neuronal death is due to the abnormal accumulation of a protein called amyloid in the brain of Alzheimer’s patients, resulting in the form of aggregates in the form of amyloid plaques. around neurons.
Accumulating amyloid causes neuroinflammation, characterized by the production of cytokines, and oxidative stress, characterized by the production of free radicals.
These two phenomena would in turn increase the formation of plaques.
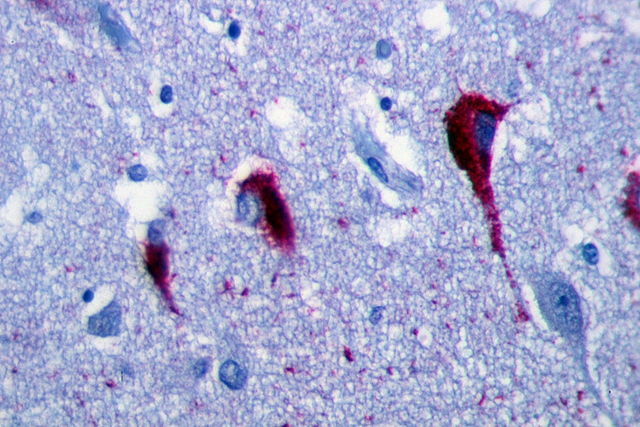
On the other hand, Alzheimer’s disease is characterized by neurofibrillary degeneration (NFD) which is characterized by lesions affecting the interior of neurons.
These DNFs are formed from an accumulation of a protein called tau protein which is present in an abnormal form.
Section of tissue showing Tau proteins appearing in an abnormal form and accumulating inside the neurons of a person suffering from Alzheimer’s disease.
These lesions are distributed throughout the brain, but predominate in the hippocampus and entorhinal cortex, a brain structure involved in memory storage.
Amyloid accumulation can occur 10 to 15 years before the first symptoms of Alzheimer’s disease, while tau protein begins to accumulate in the neocortex 3 to 5 years before the first symptoms.
Changes in amyloid and tau levels can be detected in cerebrospinal fluid, as well as by neuroimaging techniques (e.g. imaging using an amyloid-scoring probe).
The disease is also characterized by neuronal loss at the cortical level and a marked drop in acetylcholine, the neurotransmitter involved in memory.
Screening
Extensive efforts have been made to identify biomarkers in cerebrospinal fluid and blood. The measurement of the ratio between the tau protein and the amyloid protein in the blood is a reliable indicator of a pathology in subjects suffering from Alzheimer’s disease, but also in those who have not yet developed the disease.
Neuroimaging (e.g., positron emission tomography, MRI) is used to monitor disease progression, determine severity, and measure the effectiveness of treatment.
The use of a probe marking amyloid makes it possible to follow the accumulation of this protein and to identify the individuals who will develop the disease years later.
The evolution of Alzheimer’s disease is slow, with stages associated with different types of common behaviors.
It affects most areas of your brain. The disease can affect memory, thinking, judgment, language, problem-solving, personality, and movement.
The course of Alzheimer’s disease distinguishes five phases: preclinical Alzheimer’s disease, mild cognitive deficit (decline) due to Alzheimer’s disease, mild dementia due to Alzheimer’s disease, moderate dementia due to Alzheimer’s disease and severe dementia related to Alzheimer’s disease.
As a reminder, dementia is a term used to describe a group of symptoms that affect the patient’s intellectual and social abilities enough to interfere with daily function.
Although Alzheimer’s disease theoretically has five stages, it is important to know that these stages are only rough generalizations. The disease is a continuous process. Each person has a different experience of Alzheimer’s disease and its symptoms.
Alzheimer’s disease in the preclinical stage
Alzheimer’s disease begins long before any symptoms appear. This stage is called preclinical Alzheimer’s disease and it is usually identified only in research settings. Neither the patient nor those around him notice any symptoms during this stage.
This phase of evolution of Alzheimer’s disease can last for years or even decades. Although no changes are seen, new imaging technologies can identify deposits of a protein called beta-amyloid, a hallmark of Alzheimer’s disease. The ability to identify these early deposits may be particularly important for clinical trials and in the future as new treatments are developed for Alzheimer’s disease.
Additional biomarkers – measures that may reflect an increased risk of disease – have been identified in Alzheimer’s disease. These biomarkers can be used to support the diagnosis of Alzheimer’s disease, usually after symptoms appear.
Genetic testing can also tell you if one has a higher risk of Alzheimer’s disease, especially early-stage Alzheimer’s disease. These tests are not recommended for everyone, but the doctor can determine if these genetic tests may be helpful.
As with new imaging techniques, biomarkers and genetic testing will become increasingly important as new treatments for Alzheimer’s disease are developed.
Mild cognitive impairment due to Alzheimer’s disease
People with mild cognitive impairment (MCI) experience slight changes in their memory and ability to think. These changes are not significant enough to affect work or relationships. People with MCI may have memory lapses for information that is usually easily remembered, such as conversations, recent events, or appointments.
These individuals may also have difficulty estimating the time required to complete a task or correctly assessing the number of steps required to complete a task. The ability to make good decisions may become more difficult.
Alzheimer’s disease is not associated with mild cognitive decline which is often diagnosed based on a doctor’s review of symptoms. However, the tests used to identify preclinical Alzheimer’s disease can be used to determine if the MCI is due to Alzheimer’s disease or something else.
Alzheimer’s disease is often diagnosed in the mild dementia stage, when it becomes apparent to family and doctors that a person has significant problems with memory and thinking that affect day-to-day functioning.
People may experience:
Loss of memory of recent events. Individuals may have particular difficulty remembering newly learned information and tend to ask the same question over and over.
Difficulty solving problems, complex tasks and good judgments. Planning a family event or balancing a checkbook can become overwhelming. Many people show poor judgment, for example when making financial decisions.
Personality changes. People may withdraw – especially in socially difficult situations – or show unusual irritability or anger. Reduced motivation to complete tasks is also common.
Difficulty organizing and expressing thoughts. Finding the right words to describe objects or express ideas clearly becomes more and more difficult.
Getting lost or misplacing property. Individuals are finding it increasingly difficult to find their way around, even in familiar places. It is also common to lose items, including valuables.
Moderate dementia due to Alzheimer’s disease
As the disease progresses to moderate dementia, people become more confused and begin to need more help with daily activities and self-care.
People with the moderate dementia stage of Alzheimer’s disease may:
Exhibit increasingly poor judgment and increasing confusion. Individuals lose track of where they are, the day of the week or the season. They may confuse family members or close friends or confuse strangers with their family.
They may wander, possibly in search of more familiar surroundings. These difficulties make it dangerous to leave people with moderate dementia alone.
Memory loss is even greater. People may forget details of their personal history, such as their address or phone number, or the location of the school they attended. They repeat their favorite stories or make up stories to make up for their memory loss.
Need help with some daily activities. Assistance may be required in selecting appropriate clothing for weather conditions, as well as with bathing, grooming, using the restroom and other personal care.
Significant changes in personality and behavior. It is not uncommon for people in the moderate stage of dementia to have unfounded suspicions – for example, they convince themselves that friends, family members or professional caregivers are robbing them or that their spouse is having an affair. Others may see or hear things that aren’t really there.
Individuals often become restless or restless, especially late in the day. Some people may have outbursts of aggressive physical behavior.
Severe dementia due to Alzheimer’s disease
When the progression of Alzheimer’s disease leads to the stage of severe dementia, mental function continues to deteriorate and the disease has an increasing impact on physical abilities and movements.
In advanced stages of severe dementia due to Alzheimer’s disease, people:
Lose the ability to communicate coherently. She no longer speaks sensibly, although she can sometimes speak words or phrases.
Need daily personal care assistance with eating, dressing, using the bathroom and all other daily personal care tasks.
Show a decline in their physical abilities. They are unable to walk without assistance, sit up or raise their head without support. Muscles may become stiff and reflexes abnormal. Eventually, a person loses the ability to swallow and control bladder and bowel functions.
Practical case
In September 2006, a 76-year-old man, a worker by profession, came to consult a geriatrician for memory problems accompanied by depressive symptoms (he suffered from bereavement for his sister).
This visit follows a surgical operation (January 2006) and a visit to a psychiatrist (May 2006).
During the episodic memory evaluation test (Grober and Buschke test) consisting in learning and retaining a list of 8 words (the Grober and Buschke test in its long version), the patient commits two intrusions (the patient names words that are not on the list). Moreover, passing the clock test), seems to evoke a semantic problem, despite correct visual and spatial ability.
The doctor hypothesizes a deficit of the brain structures involved in episodic memory (hippocampus) because the patient has a problem during encoding (encoding is the first stage of memory. The information obtained by a stimulus is memorized before being stored).
Despite fluent speech, semantic fluency is low with a score of 12 words, suggesting abnormal frontal and temporal structures of the dominant left hemisphere for language. In addition, the patient scored poorly on the working memory assessment test.
On the other hand, the patient does not suffer from apraxia, attention disorder, manages to conceptualize and orients himself well in time and space.
A year later, the patient consults the geriatrician again following the concerns of his wife who finds him apathetic and detached from the joys of everyday life. Neuropsychological tests are carried out. The patient has difficulty naming the day of the week and the month (temporal disorientation).
Episodic memory (Grober and Buschke test): the patient has a problem during encoding. He has difficulty remembering words that have just been presented to him (immediate recall). In addition, the patient this time commits eight intrusions. The neuropsychologist decides not to carry out the two other parts (ie interfering test and deferred recall) of the test in order not to aggravate the state of anxiety in which the patient finds himself. The neuropsychologist hypothesizes that the patient suffers from short-term memory problems affecting the temporal lobe.
Executive functions: the patient has difficulties with conceptualization and planning according to the Rey Figure test 3. His literal fluency is weak.
The neuropsychologist hypothesizes that the patient suffers from executive function disorders affecting the frontal lobe.
3 The Rey figure test is a quick test consisting in reproducing from memory a complex geometric figure with no obvious meaning. It assesses the perceptual activity of the person (whether a teenager or an elderly person), as well as his memory and attention.
Moreover, despite a good understanding of sentences and fluent speech, the patient has difficulty naming the objects presented to him on cards, confirming impairment of the frontal and temporal areas of language in the left hemisphere.
Finally, his wife thinks that her husband has difficulty living in everyday life (running errands, paying bills).
Following these observations, a diagnosis of possible Alzheimer’s disease is made.
Life expectancy varies for each person with Alzheimer’s disease. It is seven to ten years for patients diagnosed at age 60.
What is the average life expectancy of Alzheimer’s disease?
Alzheimer’s disease can also remain undiagnosed for several years. The average time between the onset of symptoms and the diagnosis of the disease is 2.8 years.
The effect of treatment
Treatment will not prevent disease progression. It is also unclear whether the treatment can prolong a person’s life. Ultimately, Alzheimer’s disease will progress and take its toll on the brain and body. As it progresses, the symptoms and side effects will get worse.
However, a few drugs can slow the progression of Alzheimer’s disease for at least a short time. Treatment can also improve the patient’s quality of life and help alleviate certain symptoms.
What factors affect longevity in patients with Alzheimer’s disease?
Several factors influence a person’s life expectancy.
The age of diagnosis. The age at which you are diagnosed with Alzheimer’s disease can have the greatest impact on your life expectancy. The earlier you are diagnosed, the longer you can live. American researchers (Hopkins School of Public Health) found that the average life expectancy of people diagnosed at age 65 was 8.3 years, while that of people diagnosed at age 90 was 3.4 years.
Gender: A 2004 study found that men lived an average of 4.2 years after initial diagnosis. Women lived an average of 5.7 years after their diagnosis.
The severity of symptoms: People with a motor impairment or behavioral disorder such as falling and a tendency to wander or move away, had a shorter life expectancy.
Brain abnormalities: The study also showed a link between brain and spinal cord abnormalities and the length of life.
Other health issues: People with heart disease, a history of heart attack, or diabetes had shorter lifespans than patients without these complicated health factors.
According to another team of researchers, three factors really seem to matter: age at first symptom (older people die faster), gender (men live shorter) and degree of deficit at diagnosis.
A formula to predict the life expectancy in Alzheimer’s disease
Using these three factors, they came up with a simple formula to predict patients’ risk of death. Then, based on these risk levels, patients were divided into four life expectancy categories.
People in the last quarter lived between four and a half and nine years, or about seven years on average, from diagnosis. Those in the first quarter lived between about a year and nine months and five years, averaging about three years.
For example, according to the formula, an 82-year-old woman with mild to moderate dementia should live five years after diagnosis. A 63-year-old man with mild dementia at diagnosis is expected to live for seven years.
« A difference in survival of two to four years can be extremely important for planning the budget necessary for the care of the patient, » says the researcher.
Pneumonia is a common cause of death, caused by swallowing problems that allow food or drink to enter the lungs, where infection can occur.
Dehydration, malnutrition, falls and other infections are other common causes of death.
Alzheimer’s disease is responsible for several symptoms (i.e. what the patient feels) and is characterized by clinical signs that can be observed by relatives and the doctor.
Some warning signs are often insidious: changes in weight, behavior, language, walking, and sleep, as well as the occurrence of repeated falls.
Signs and Symptoms of Alzheimer’s Disease
Recent memory loss
Memory problems are the symptoms that constitute the main reason for consultation, on the initiative of the patient or more frequently that of the family. Indeed, the patient tends to minimize or deny his troubles. Memory difficulties relate to recent facts and then to old facts. It is the so-called episodic memory that is mainly affected. For example, people with Alzheimer’s disease will often forget to go to an appointment (if it is a frequently recurring event). According to a study published in 2015, women with memory trouble have an increased risk (+70%) of developing dementia from the age of 65.
Difficulties performing daily tasks
People will have difficulty performing familiar everyday tasks that do not require special effort (eg using a household appliance).
Difficulty expressing oneself and finding the right words.
A person with Alzheimer’s disease often forgets simple words. For example, she will ask for « the thing to eat » rather than the fork.
Difficulty orienting oneself in space and time.
The person with Alzheimer’s disease can get lost in their own street, no longer know where they are and no longer be able to return home.
Difficulties in passing judgment.
People with Alzheimer’s can dress without paying attention to the outside temperature. In addition, they lack discernment in matters of money and may be victims of abuse.
Difficulties in handling abstract notions.
A person with Alzheimer’s disease loses track of numbers or what they represent. For example, she doesn’t know what the numbers on a bank statement or a street sign represent.
Difficulty finding lost items.
A person with Alzheimer’s disease will store things in an inappropriate place. For example, keys in a fridge or a watch in a shoebox.
Depressive and behavioral disorders.
A person with Alzheimer’s can quickly change mood and go from a serene state to crying or angry outbursts, for no apparent reason. Numerous studies have even shown that nearly 90% of patients suffering from Alzheimer’s disease also present with mood disorders, agitation, and loss of appetite. According to their authors, these results suggest that these disorders occur years before the diagnosis of dementia. Patients with Alzheimer’s disease also presented behavioral problems earlier: loss of appetite, apathy, irritability, etc.
Personality changes.
A person with Alzheimer’s can quickly become very confused, fearful or suspicious of someone close to them.
Loss of interest. The person with Alzheimer’s may become passive and spend hours doing nothing (eg watching television for hours, sleeping more than normal, and not going outside).
In summary, Alzheimer’s disease results in cognitive and non-cognitive (ie psychological and behavioral) symptoms that impair activities of daily living.
The two forms of Alzheimer’s disease symptoms
Symptoms can be divided into two classes: cognitive symptoms and psychological and behavioral symptoms.
Cognitive symptoms
Memory problems: the person has problems retrieving information stored in their brain. This incapacity is compensated for at the start of the disease thanks to the work of certain parts of the brain which remain intact (in particular the frontal lobe), but is gradually accentuated as the disease worsens.
Initially limited to the years preceding the disease, retrograde amnesia gradually spreads until reaching the earliest memories and even the identity of the patient, who has more and more difficulty recognizing his relatives. Amnesia affects both episodic memory (the patient’s own memories) and semantic memory (knowing how to name objects or images, having verbal fluency, etc.). Working memory is generally impacted at the onset of the disease: patients have difficulty performing simultaneous tasks.
Semantic memory deficits generally occur later than episodic memory disorders. This translates into difficulty in saying as many words as possible beginning with a given letter (poor verbal fluency), in making paraphasias (e.g. saying table instead of desk), in responding in a more general way (by say animal for dog) and to experience problems of categorical classification (the patient has trouble guessing which of the fir tree or the palm tree is semantically closest to the pyramid).
Visual and spatial disorders
Language disorders: they are linked to semantic memory disorders and can be early. At the beginning of the disease, they are most often characterized by a lack of words which alters spontaneous speech: patients often try to circumvent the obstacle by using circumlocutions. At this stage there is generally no phonemic or syntactical disturbance or comprehension disturbances and speech is normal. At a more advanced stage, paraphasias are numerous. We observe perseverations on a word or a syllable, or around a theme. Logical word order disappears in speech, and listening comprehension is disrupted. On the other hand, written language can be affected, with spelling difficulties.
Finally, in the severe stage of the disease, spontaneous production is greatly reduced, or even non-existent. It may be limited to echolalia. The language is misunderstood. This is called global aphasia.
Practical disorders (apraxia)
Loss of recognition of objects, faces (agnosia) .
Impaired executive functions and judgment. Disorders of executive functions are manifested by difficulties in abstraction, reasoning, mental flexibility and planning.
Psychological and behavioral symptoms
Depressive symptoms
Loss of initiative and interest
Indifference
Anxiety, often associated with depression.
Irritability
Hustle
Aggressive
Delusions (ideas of persecution, jealousy)
Hallucinations (mainly visual)
Sleeping troubles
Wanderings (severe stage)
Runaways
Confusional episodes (in moderate and severe stages).
Disinhibition
Repetitive motor behaviors
Eating Disorders
What are the signs that should worry us?
There are reasons for concern when a person:
cannot do two things at once (e.g. cook dinner);
wanders off on a familiar path;
forgets the names of relatives;
no longer recognizes the faces of relatives;
rehashing the same questions.
A consultation is necessary if the person:
no longer knows how to perform certain daily tasks (eg operate a washing machine);
gets lost in family ties;
no longer knows the function of certain objects;
puts things away in inappropriate places.
On the other hand, there is no cause for concern when the person:
no longer knows where she parked her car;
forgets to call someone back;
forgets the name of a person she has just met;
no longer knows where to put an object;
can’t remember a word.
Other possible warning signs
Anosognosia
Patients suffering from Alzheimer’s disease have little or no awareness of their disease: this is called anosognosia . It complicates patient care and increases the caregiver’s burden. This would be one of the possible warning signs.
Mild behavioral disorder (deficit): one of the precursor symptoms of Alzheimer’s disease
Researchers have compiled a list of behavioral symptoms to help identify those at risk, assuming that certain behavioral changes may be a warning sign of Alzheimer’s disease. Experts have long emphasized that mild cognitive impairment is an early warning sign of Alzheimer’s disease. Now, some of them are pushing a new concept they call “mild behavioral (deficit) disorder,” describing persistent abnormal changes in an older person’s behavior. Changes include issues such as social withdrawal, tantrums, anxiety, and obsession.
“We are not talking about a jolt in someone’s behavior but about abnormal and persistent behavior. it would be the first sign that something is wrong in the brain,” says the lead author of the study.
He and his colleagues developed a symptom checklist that doctors could use to assess patients with behavioral problems. The tool needs to be refined, however, as the research presented at the Alzheimer’s Disease Conference is preliminary.
“People often think that Alzheimer’s disease is primarily a problem of memory loss. However, many patients with dementia also have neuropsychiatric symptoms – an umbrella term encompassing behavioral problems and mood and perceptual disturbances”.
According to the researcher, it is important for doctors that families can realize that lasting changes in behavior can be a warning sign.
Here is a list of symptoms of mild behavioral disorder:
decreased motivation which refers to apathy or a lack of interest in things in which individuals had an interest. For example, a grandparent no longer seems interested in the lives of his grandchildren. Apathy appears in 25% to 50% of patients, depending on the study;
emotional symptoms such as depression, anxiety and irritability;
difficulty controlling impulses that manifests as restlessness, obsession, or even habits like gambling;
problems with perception, with the presence of delusions or hallucinations. Older people have a mild behavioral problem if they have any of these symptoms, periodically, for at least six months.
Researchers estimate that 13% of older people with mild cognitive impairment will develop dementia within a year. This percentage rises to 25% if there is also the presence of mild behavioral problems.
Currently, there are no treatments that can prevent or permanently treat the symptoms of Alzheimer’s disease. However, early detection allows for available treatments and support services as soon as possible. When it comes to behavioral issues, there are ways to deal with them. In some cases, a minor change in a person’s environment can help. Some people can be treated with medications such as antidepressants or anti-anxiety medications under the supervision of a doctor. Source: Alzheimer’s Association International Conference, Toronto, July 2016.
In 2015, a study conducted by American researchers (Washington University School of Medicine, Saint-Louis) already indicated that behavioral disorders could be present before memory problems. The authors describe these disorders with, in order of appearance:
irritability,
depression,
sleep disturbances,
anxiety,
change in appetite,
restlessness and apathy,
exaltation,
motor disorders,
hallucinations,
the illusions and
disinhibition.
To reach this conclusion, the authors of the study analyzed the files of 1218 people who had initially consulted without signs of Alzheimer’s disease, before the latter does not start thereafter. Source: “Noncognitive” symptoms of early Alzheimer disease. Neurology, January 2015.
However, a study published in JAMA Psychiatry in 2017 does not support the idea of personality change before the onset of mild cognitive impairment or dementia.
According to the lead author of the study:
We found that the personality remained stable even in the last years before the onset of the disease.
The researchers analyzed the personality and cognitive performance of more than 2,000 individuals who had no cognitive deficit before the study. About 18% of study participants later developed cognitive impairment or dementia.
What the researchers found was that the trajectory of personality traits did not differ between those who would later develop dementia and those who remained without cognitive problems.
While personality change was not an early sign of dementia, the study further supports the fact that personality traits (eg high emotionality or low level of conscientiousness) are risk factors for dementia. Source: A. Terracciano et al. Personality Change in the Preclinical Phase of Alzheimer’s Disease. JAMA Psychiatry, September 2017.
Oral expression
American researchers have tried to detect the first signs and symptoms of Alzheimer’s disease in Ronald Reagan, by studying his press conferences when he was President of the United States of America. The texts have been compared to those of George HW Bush Sr. Responses to press conferences have the particularity of requiring a significant cognitive effort because they must be spontaneous.
Ronald Reagan was diagnosed with Alzheimer’s in 1994, five years after he left the presidency of the United States. He had been regularly followed by his doctors during his two presidential terms. His remarks made during public conferences have in particular been closely scrutinized. For example, during a debate with his opponent W. Mondale in 1984, he had confused the place where was with the federal capital (Editor’s note which can be seen as a slip). Arizona State University researchers noticed subtle changes between his first and second terms when they compared excerpts from his press conferences with those of George HW Bush, the two being around the same age. at the beginning of their mandate (69 years old for Reagan in 1981, 64 years old for Bush in 1993). Using an algorithm, they studied the changes in the modes of expression of the two presidents. This algorithm had been used to analyze novelists’ writing changes.
Results: Ronald Reagan tended, towards the end of his presidency, to repeat the same word and to use imprecise words (example “thing”), contrary to his successor George Bush who did not develop Alzheimer’s disease.
The researchers point out, however, that this algorithm should be tested on a large number of people in order to validate it scientifically. As a reminder, difficulties in finding the right words are one of the main warning signs of the disease. Thus, a person with Alzheimer’s disease no longer remembers simple words (“eg knife”) and will replace them with an expression (“the thing to cut”). This is difficult to detect at the onset of the disease, because the patient masks his condition by using carefully repeated sentences and simple words. This algorithm had previously been used on the writings of Agatha Christie, suspected of having suffered from Alzheimer’s disease, as well as on those of the British writer Iris Murdoch, suffering from the disease.
Alzheimer’s: altered signs in brain activity
A French study (Pitié-Salpêtrière, Paris, France) aims to identify early the first signs and symptoms of Alzheimer’s disease in 400 people aged 70 and under and in good mental health. Participants will have to pass cognitive tests in the form of mental exercises. In parallel, the electrical activity of the brain – more precisely the cerebral cortex – is recorded by electroencephalography (EEG).
The slightest change in brain activity could be interpreted as a sign of a loss of synaptic connections and gray matter, characteristic of the onset of Alzheimer’s disease.
The interest of the study, called Insight, is therefore to identify the patient before he is in a prodromal state, that is to say before the first symptoms become detectable by neuropsychological tests. To do this, the researchers hope to be able to identify symptoms and warning signs of Alzheimer’s disease before the prodromal stage. The 400 participants will take cognitive tests every five years (twice a year) (memory, attention, executive functions, language, praxis, etc.).
Neuropsychologists try to distinguish the disorders that normally appear during aging from those that should alert, in particular the difficulty of memorizing a newly acquired word or a new event (we speak of anterograde amnesia). While performing their mental exercises, researchers place electrodes on individuals’ skulls to perform an EEG. According to the researchers, “Alzheimer’s disease alters the EEG at rest and during exercise. These subtle changes are the consequence of a loss of neurons and synapses (areas of contact between neurons). A blood test will be taken at the same time.
When a case of Alzheimer’s has declared itself, the blood samples will be analyzed to identify biological markers likely to be involved in the pathology of the disease. Finally, the individuals are subjected twice a year to a magnetic resonance imaging (MRI) examination, which will make it possible to visualize any brain lesions, in particular in the hippocampus – an area involved in memory. It is estimated that the volume of the hippocampus decreases by more than 4% per year in Alzheimer’s patients, compared to only 1% in healthy subjects.
Slower walking
Older people who walk more slowly have higher amounts of amyloid in their brains, a French study has found. Researchers have reported an association (albeit a modest one) between higher levels of amyloid plaques in the brain and slower walking speed in older adults. Amyloid is a protein that accumulates – in the form of plaques – in the brain of Alzheimer’s patients.
« These results suggest that people with Alzheimer’s disease show subtle signs of gait disturbances, in addition to well-known symptoms such as memory complaints, even in those with a normal gait rhythm, » said Dr. lead author of the study (University of Toulouse).
This study, which allowed researchers to look at participants at a specific point in time, only established an association between brain amyloid levels and walking speed, but not a causal relationship between the two. The research team analyzed 128 people (average age: 76) who had no formal diagnosis of dementia, but were considered high risk due to memory problems. Almost half had abnormally high levels of amyloid plaque in their brains (48%) and mild cognitive impairment (46%). Gait speed was measured using a standard synchronization test (transition from brisk walking to usual walking pace). Amyloid accumulates in several regions of the brain,
“The way we walk is controlled by areas of the brain that define rhythm. When this part of the brain does not work properly, it can have an impact on walking or speed, ”explains an Alzheimer’s disease specialist.
However, it is important to reassure older people who walk slower than others. In 2012, American researchers (Boston Medical Center) also studied the association between walking and cognitive performance in 2,140 volunteers aged 62 on average. They had started from the hypothesis that difficulty in walking and walking speed are warning signs of symptoms characteristic of Alzheimer’s disease. Their results reported a link between walking speed and the onset of dementia. This association has to date no scientific explanation. Source: Del Campo N et al. MAPT/DSA Study Group. Relationship of regional brain β-amyloid to gait speed. Neurology. 2016 Jan 5;86(1):36-43.
Alzheimer’s: brain imaging to confirm the symptoms of Alzheimer’s disease
Signs of brain damage can appear well before the first symptoms in healthy individuals whose parents both have Alzheimer’s disease.
“When the diagnosis is made, it is already too late,” says Dr. Lisa Mosconi (New York University School of Medicine). “This is why it is necessary to detect the signs of the disease in these people at risk before the first symptoms”.
52 subjects aged 32 to 72 underwent neuroimaging examinations – including positron emission tomography and magnetic resonance imaging – which visualize amyloid plaques and brain activity.
Results: Individuals whose parents had Alzheimer’s disease had more amyloid plaques and a lower brain volume, compared to those whose parents had no pathology.
“Our study suggests the existence of predisposition genes that promote lesions characteristic of Alzheimer’s disease in individuals at risk. It remains to be determined which ones. Source: Brain imaging of cognitively normal individuals with 2 parents affected by late-onset AD. Neurology, 2014.
Analysis of the structure by MRI is characterized by atrophy in the temporal cortex (in particular the hippocampus) and the parietal cortex, with an accentuation of the sulci.
Imaging confirms or not the diagnosis of the presence of symptoms characteristic of Alzheimer’s disease and allows the doctor to decide to prescribe a drug.
Accentuation of furrows: one of the diagnostic signs of Alzheimer’s disease
Sleep problems
An experiment conducted on mice suggests that sleep disturbance could be one of the early signs of Alzheimer’s disease. In the study published in Science Translational Medicine (Sept. 2012), the researchers showed that the sleep cycle was disrupted when amyloid plaques appeared in the brains of these mice. As a reminder: amyloid plaques are characteristic lesions of Alzheimer’s disease; Researchers have succeeded for fifteen years in “manufacturing” transgenic mice which develop these lesions as they age. It is important to detect early warning signs of the disease well before the appearance of the first symptoms (loss of short-term memory).
« If sleep problems at the very beginning of the disease, these signs and symptoms could serve as a means of detecting Alzheimer’s disease », explains one of the authors of the study who adds: « we do not yet know in what form These sleep disorders appear: reduction in sleep time, difficulty in falling asleep…”.
Frequent falls
People with lesions characteristic of Alzheimer’s disease (deposits of amyloid plaques and tau proteins) see their risk of falling multiplied by 3 when they practiced an activity of daily living. These results come from an American study of 125 people (average age: 74 years) whose number of falls was evaluated for one year. Amyloid deposits and elevated levels of tau protein were measured in cerebrospinal fluid after lumbar puncture. Source: Neurology, July 30, 2013.
The causes that may explain these falls are numerous and associated with other signs and symptoms of Alzheimer’s disease:
Deficit in cognitive faculties (judgment, attention).
Screening tests are being developed for early detection of developing Alzheimer’s disease to allow people at risk to receive treatment early before it is too late.
One of the reasons cited by the scientific community for the high failure rate of clinical studies is that it is virtually impossible to treat patients once symptoms are present.
Screening for Alzheimer’s disease by detecting amyloid in the blood
Researchers have developed blood tests that identify the amyloid protein in its abnormal form.
Recent research shows that a simple blood test could help detect who might develop Alzheimer’s disease. Researchers were able to develop a blood test to measure the amount of amyloid in a person’s brain.
The abnormal shape of the protein is characterized by a modification of its structure which ends up aggregating. This abnormal buildup of amyloid appears about 17 years before symptoms of dementia occur.
This screening test has a reliability of just over 90% when combined with age or the presence of the APOE epsilon 4 allele (APOE4), a genetic risk factor (in 9 cases out of 10, a positive test is confirmed later).
The test would make it possible to identify people at risk of developing Alzheimer’s disease and to refine the diagnosis by lumbar puncture or by positron emission tomography.
Source: Wolters FJ et al. Hemoglobin and anemia in relation to dementia risk and accompanying changes on brain MRI, Neurology, July 2019; A. Nabers et al. Amyloid blood biomarker detects Alzheimer’s disease.EMBO Molecular Medicine (2018) e8763.
Antibodies as screening tools for early detection of Alzheimer’s disease
In 2016, another team used antibodies as biomarkers to detect people with mild cognitive impairment, a stage leading to Alzheimer’s disease but also to other pathologies such as vascular diseases.
The researchers selected 50 antibodies produced by the immune system as being most likely to detect the disease.
They then tested them on 236 people, 50 of whom had mild cognitive impairment.
According to the experiments carried out, the test made it possible with 100% accuracy to determine people with mild cognitive impairment leading to Alzheimer’s disease.
These results must be confirmed before the test is put on the market.
Early detection of Alzheimer’s disease-specific proteins
In a study published in 2014, a blood test identified 10 disease-specific proteins. 1,148 individuals participated in this study, of which 476 of them had Alzheimer’s disease, 220 had mild cognitive impairment and 452 were in good cognitive health. Of the thousands of proteins found in the blood, 26 have been linked to Alzheimer’s disease, and 16 to brain atrophy (reflecting loss of neurons).
“We have 10 proteins that can predict whether a person with mild cognitive impairment will develop Alzheimer’s disease one year later, with a high level of reliability (87%),” says the study’s lead author.
This test would be used to identify patients at a very early stage of the disease and include them in new clinical trials, in order to increase the chances of developing effective treatments capable of slowing down or even stopping the progression of the disease.
“The next step will be to confirm these results and develop a reliable screening test for Alzheimer’s disease that can be easily used by doctors,” concludes the group of researchers.
Source: Abdul Hye et al. Plasma proteins predict conversion to dementia from prodromal disease. Alzheimer’s & Dementia, July 2014.
Some lipids would also be good indicators
A team of American researchers (Georgetown University) evaluated a test in adults in their seventies in good mental health. They measured the levels of 10 lipids in their blood.
Measuring the levels of these lipids makes it possible to identify, with 90% reliability, those who will develop cognitive impairment over a period of two to three years.
This means that in 9 out of 10 cases, a person with a positive test will suffer from mild cognitive decline or Alzheimer’s disease.
The main author of this research recalls that blood tests are much easier to perform than current tests that involve neuroimaging techniques or cerebrospinal fluid sampling.
The study followed, for 5 years, 525 participants in their 70s in good health, of whom 74 participants were diagnosed with Alzheimer’s disease or amnesic mild cognitive impairment.
Source: Medicine Plasma phospholipids identify antecedent memory impairment in older adults. Nature, March 2014.
A test using DNA
German researchers are planning to develop a blood test for early detection of Alzheimer’s disease.
They identified 12 fragments of microRNA* (or micro ribonucleic acid) which would be characteristic of Alzheimer’s disease.
MicroRNAs are short pieces of RNA that regulate gene expression. As a reminder, RNA is produced from DNA in cells to make proteins.
The reliability of the test is 93%, that is, 93% of the positive screens were found to be accurate.
202 blood samples were analyzed. This blood test will have to be validated with a larger sample.
. Source: Genome Biology journal, July 29, 2013.
Neuroimaging for screening for early detection of Alzheimer’s disease
Swiss researchers have deciphered how different areas of the brain interact with each other in healthy subjects (September 2015).
Using the technique of neuroimaging, they identified thirteen main networks that activate in the brains of these participants. This activation takes place with certain coordination.
These results could have an impact on the detection of Alzheimer’s disease, knowing that it is characterized by a disruption of neural networks located in certain parts of the brain, before the appearance of the first symptoms.
Eye examination
Scottish computer scientists (University of Dundee) will develop, in the spring of 2015, software called VAMPIRE (Vessel Assessment and Measurement Platform for Images of the Retina) which will take images of the vascularization of the eye.
This imaging data will be combined with medical information to establish a possible link between abnormalities in the vessels that irrigate the eye and the onset of Alzheimer’s disease.
The researchers point out that the blood circulation (veins and arteries) of the eye undergoes branching changes following the appearance of certain pathologies such as stroke or cardiovascular disease.
These abnormalities of the vascular system are characterized by a change in the morphology of the vessels, which become wider and more sinuous. They can be the beginnings of Alzheimer’s disease.
In 2014, Cognoptix, an American biotechnology company, developed an eye examination device (SAPPHIRE II) to achieve early detection of Alzheimer’s disease.
This examination would make it possible to identify a biological marker characteristic of the disease (in this case amyloid) by examining the eyes of patients, according to Carl Sadowsky, principal coordinator of clinical trials.
These studies involved 20 healthy volunteers and revealed that this test has a sensitivity of 85% and a specificity of 95% when it comes to distinguishing patients at risk from those who are not affected.
The risk of cardiovascular disease would increase in people with symptoms of depression.
The researchers studied more than 7,300 elderly people in France with no history of heart disease, stroke, or dementia at the start of the study period. About 30% of women and 15% of men had high levels of depressive symptoms.
Participants were reassessed two, four, and seven years later. At each follow-up visit, about 40% of depressed people no longer showed symptoms of depression, while the same percentage had instead developed symptoms. Less than 10 percent of participants were taking antidepressant medication.
Those who had high levels of depressive symptoms at each visit had an increased risk of heart disease or stroke within 10 years. This risk increased by 75% for individuals who had symptoms of depression at each of the four visits.
The results suggest that depression could be a risk factor for cardiovascular disease. However, they do not allow us to conclude that there is a cause-and-effect relationship.
The authors of the study (Dr Renaud Pequignot, INSERM, Paris) suggest that doctors should closely monitor people aged 65 and over with depression.
According to the World Health Organization, depression, and cardiovascular disease are the leading causes of disability and death, respectively. Depression increases the likelihood of having cardiovascular disease and vice versa.
Source: Péquignot R. et al. High Level of Depressive Symptoms at Repeated Study Visits and Risk of Coronary Heart Disease and Stroke over 10 Years in Older Adults: The Three-City Study. Journal of the American Geriatrics Society, 2016; 64 (1): 118.
Another study reported that depressive symptoms in women have been linked to a greater risk of heart disease, as up to 25% of women experience depression in their lifetimes. Such depressive symptoms may be considered an emergent, non-traditional risk factor that can increase the chances of developing cardiovascular disease (CVD).
A link between depression and stroke, a form of cardiovascular disease
Australian researchers have found that women with depression have a 2.4 times greater risk of stroke than those without « When physicians care for their patients, they need to determine the severity of their mood disorders and the long-term adverse effects they may have, » said Caroline Jackson, Ph.D., study author. and epidemiologist at the University of Queensland in Australia. “Current stroke prevention guidelines tend to overlook the potential role of depression. »
This large-scale study examined the association between depression and stroke in 10,547 middle-aged women (47-52 years old) who had to answer questionnaires about their physical and mental health. About 24% of the participants said they were depressed.
A previous study reported a 30% increased risk in participants who were on average 14 years older. Although depression is associated with an increased risk of stroke, the absolute risk of stroke remains low (2%) for this age group.
The researcher does not know the reason for the association between depression and stroke.
“Inflammatory and immune mechanisms with adverse effects on blood vessels could be the cause,” says Dr. Jackson.
Source: Depression linked to almost doubled stroke risk in middle-aged women (source: Stroke, May 2013).
In 2012, a meta-analysis published in the journal Stroke and listing 17 articles confirmed the existence of a link between the presence of depression and an increased risk (+34%) of stroke, considering the body mass index, smoking, high blood pressure, and diabetes. This correlation is similar for both men and women, although the prevalence of depression is higher in women. However, this study does not show that depression is the cause.
Depression is a modifiable risk factor for heart disease.
Another study confirms that symptoms of depression are causally linked to an increased risk of cardiovascular disease, suggesting that depression is a modifiable risk factor for heart disease.
The study involved over 10,000 English individuals whose mental state was assessed 6 times over a 20-year period.
The risk of coronary heart disease doubles when these people report depressive symptoms during at least 3 assessments.
However, no association between depression and stroke has been reported. According to the author of the study, depression is not a cause of stroke, but rather a consequence of the presence of vascular disease.
According to a meta-analysis of 68,000 English people, subjects with symptoms of psychological distress (anxiety, depression, social problems or loss of confidence) have an increased risk of death ranging from 16% (if symptoms of psychological distress are mild) to 67% (if symptoms are high).
These deaths are caused by a heart attack or stroke (and in the case of high symptoms, cancer). Researchers have hypothesized that acute stress can reduce blood flow to the heart or that depression can lead to increased levels of inflammation (source: British Medical Journal, July 2012).
The risk of heart attacks and strokes can be halved if depressive symptoms are treated before signs of cardiovascular disease appear.
This study confirms that depression increases the risk of cardiovascular disease, and emphasizes the need to treat depression before the onset of these diseases, to reduce the consequences on the heart (heart attack) and the brain (stroke).
Researchers followed 235 depressive patients for 8 years. The risk of heart attack and stroke was reduced by 48% in those who received both psychotherapy and antidepressant medication, compared to those who did not.
Source: Effect of Collaborative Care for Depression on Risk of Cardiovascular Events: Data From the IMPACT Randomized Controlled Trial. Psychosomatic Medicine, 2013; 76 (1): 29.
These changes are observed using brain imaging techniques such as magnetic resonance imaging or computed tomography.
Leukoaraiosis is not specific to a precise pathological condition. It occurs frequently in elderly patients with ischemic stroke, but also in those with hypertension, vascular dementia, intermittent claudication, or mood disorders.
Several infarcts of small vessels located in the subcortical white matter may be the cause of the condition. Patients may develop subcortical dementia syndrome.
It is estimated that almost all patients with vascular dementia (and about 30 to 50% of Alzheimer’s patients) have leukoaraiosis.
It is also associated in individuals with:
chronic kidney disease,
metabolic syndrome,
retinopathy,
coronary artery disease,
high levels of homocysteine,
low levels of vitamin B12 and
high levels of C-reactive protein (a marker of inflammation).
Diabetes
The prefrontal cortex would be particularly sensitive to leucoaraiosis which seems to reduce the speed of information processing in the individual.
Finally, leukoaraiosis is associated with an increased risk of ischemic stroke and cerebral hemorrhage, but also of cognitive decline and impaired gait and motor function, which are clinical hallmarks of subcortical vascular dementia. Up to 80% of patients with leukoaraiosis have gait disturbances.
The risk of dementia increases with the severity of leukoaraiosis.
Leukoaraiosis could be due to poor irrigation of the white matter supplied by the vessels. This poor irrigation is however insufficient to create ischemia.
Risk factors
age,
female sex,
high blood pressure,
heart disease,
type 2 diabetes,
abdominal obesity,
hyperlipidemia,
hyperhomocysteinemia,
carotid stenosis,
tobacco use,
alcoholism,
chronic kidney disease.
Some studies have found an association between leukoaraiosis and depression. Patients with leukoaraiosis is varied and includes motor deficits, frequent falls, parkinsonism and pseudobulbar syndrome.
Classification of leukoaraiosis
The Fazekas classification is one of the most widely used. in clinical practice and research. It distinguishes periventricular lesions (around a ventricle) from deep and subcortical lesions. There are 3 grades depending on the severity of the lesions.
Grade 1: minimal lesions in the form of points (punctiform) or lines. They are isolated or grouped and are less than 20 mm.
Grade 2: moderate lesions (solitary lesions and more intense areas less than 20 mm in diameter).
Grade 3: severe lesions (solitary lesions with more intense areas of more than 20 mm in diameter).
This classification distinguishes between periventricular and deep involvement.
Conclusions
Leukoaraiosis is an important risk factor for ischemic stroke and recurrent stroke as well as neurological and cognitive disorders.
Patients with leukoaraiosis therefore require special care.
Meniere’s disease is a disorder that affects the inner ear which is responsible for hearing and balance.
Ménière’s disease causes dizziness and also leads to hearing problems. Ménière’s disease usually affects only one ear.
It is more likely to occur in people in their 40s and 50s.
Ménière’s disease is chronic, but treatments and lifestyle changes can help relieve symptoms. Many people with Ménière’s disease will go into remission within a few years of being diagnosed.
The causes of Meniere’s disease
The cause of Ménière’s disease is not known, but scientists believe it is caused by changes in the fluid in the tubes of the inner ear. Other suggested causes include autoimmune diseases, allergies, and genetic mutations.
What are the symptoms of Meniere’s disease?
People with Meniere’s disease experience recurring episodes of symptoms such as dizziness, hearing loss, tinnitus (a ringing sensation in the ear), blocked or full feeling in the ear, loss of equilibrium, and headache.
Additionally, certain episodes may be accompanied by nausea, vomiting and sweating due to severe vertigo.
Generally, during episodes at least two to three of the listed symptoms will appear; however, during attack-free periods few or no symptoms may be present.
It is important to note that similar symptoms can be caused by other inner ear disorders so it is best to consult a doctor for a proper diagnosis if these symptoms are experienced.
How is Ménière’s disease diagnosed?
If you have symptoms of Meniere’s disease, your doctor will order tests to examine your balance and hearing, and rule out other causes for your symptoms.
Hearing test
A hearing test, or audiometry, is used to assess whether a person has difficulty with hearing. In this assessment, the individual wears headphones and listens to different tones of varying pitch and loudness. They are asked to indicate when they can and cannot hear a dial tone in order to identify any hearing loss.
Additionally, words will be spoken into the headset for the person to repeat so that any disparities between audio perception in each ear may be determined. Several other tests may also be performed if a problem exists in the inner ear or with the auditory nerve; these measures include electrocochleography and auditory brainstem response testing.
Balance tests
Balance tests are used to evaluate the function of the inner ear. The most common test is electronystagmography (ENG), in which electrodes are placed around the eyes and water is injected into the ear, and involuntary eye movements are tracked for abnormalities.
Rotary chair tests can also be used to detect if there is a problem in the ear or brain that may be causing balance issues.
The Vestibular Evoked Myogenic Potentials (VEMP) test assesses the sound sensitivity of the vestibule of the inner ear while posturography tests help to determine which part of the balance system isn’t working properly by challenging individuals to stand and respond safely with a harness.
Other tests
Brain diseases, such as multiple sclerosis (MS) or brain tumors, can cause symptoms similar to Ménière’s disease. Your doctor may order tests to rule out these conditions, and others. They may also order a brain MRI or cranial CT scan to assess possible disorders.
Meniere’s disease treatment
Ménière’s disease is a chronic, incurable disease. However, there is a range of treatments that can help relieve your symptoms, ranging from medication to surgery for the most severe cases.
Medications
There are a variety of treatments available to help manage Ménière’s disease and reduce its symptoms. Your doctor may recommend motion sickness medications to ease dizziness, nausea, and vomiting.
If fluid buildup is causing your inner ear problems, diuretics can be prescribed to help reduce the amount of fluid in your body. For more severe vertigo symptoms, a medication injection into your middle ear may be recommended as well.
Vestibular rehabilitation exercises can improve the symptoms of vertigo. These exercises help your brain consider the difference in balance between your two ears. A physical therapist can teach you how to perform these exercises.
Hearing aids
An audiologist can treat hearing loss, usually by fitting you with a hearing aid.
Operation
Most people with Ménière’s disease do not need surgery, but it is an option for those who have severe attacks and have not benefited from the effects of other treatments.
What is the effect of diet on Meniere’s disease?
Changing your diet can help reduce the amount of fluid in the inner ear and relieve symptoms. Foods and substances to limit or exclude from your diet include:
this
caffeine
chocolate
alcohol
glutamate monosodique
It’s also important to drink six to eight glasses of water a day so your body doesn’t retain fluid.
What lifestyle changes can relieve the symptoms of Ménière’s disease?
Lifestyle changes, aside from dietary changes, that may help improve your symptoms include:
rest during vertigo attacks
eat regularly, to help regulate fluids in your body
managing stress and anxiety through psychotherapy or medication
It is also important to quit smoking and avoid any allergens. Nicotine and allergies can make Meniere’s disease symptoms worse.
What is the outlook for people with Ménière’s disease?
Although there is no cure for Ménière’s disease, there are many strategies you may want to consider to reduce your symptoms. In most people, spontaneous remission is common, although it may take years. Your doctor can help you find a treatment that’s right for you.