Cancer is nothing short of a plague to the human race, and at the current rate still has no definitive cure in sight. It’s difficult to discuss cancer survival rates as many people don’t succumb in the short term but often fall to this victim in a longer standing.
When a cancer of any nature is involved, a prevention would be far preferable to a cure. To many scientific bodies, Peto’s paradox stands as an interesting avenue of research which could potentially shine some light on methods to prevent cancer in the first place.
What Is Cancer?
In the simplest form possible, cancer is a series of errors and mutations in cell reproduction. Mutations which at a point can bypass the cell’s standard built self-destruct kill switch known as apoptosis and force cells to duplicate and grow wildly. While the body does for the most part pick up on these genetic errors, cancer is a numbers game.
With an average of 300 billion cells being replaced every single day in your body, the miniscule chance of all the correct mutations coming to light in a single cell to cause cancer, suddenly become a lot more realistic. Now that we have a basic understanding of what cancer is, we can explore what Peto’s paradox is and how it may hold some secrets into the prevention of cancer.
Peto’s Paradox
When looking at the number of cells in an animal of any kind, it would make sense that the more cells and the longer the lifespan would mean more cell duplication and more potential for errors. This all meaning, the bigger the animal, the more prone it should be to developing some kind of cancer. Strangely, this is not the case.
As it stands, humans seem to be in the unfortunate sweet spot for cancer. The majority of animals smaller than us tend to get cancer at a rate similar to us, while larger animals are less prone to any type of cancer. Horses do get cancer at a rate close to half that of humans, going even bigger, cancer in elephants is less than a quarter of that for humans. While there has not been enough research to factually state, from what research there is, it seems as though cancer in a bowhead whale is almost unheard of.
What Does This Mean For Us
That’s just the thing, we don’t know yet. Research is still being done as to why large animals don’t get cancer like humans do, once we know why, we can try to figure out how we can use this to hopefully suppress cancer in humans. At the moment, there are a few leading theories:
Cell structure – Not a single point on its own, the particular cell structure ties well into metabolism rates. The main idea being that a particular cell structure could help suppress cancer
Hyper tumours – This relies on the idea that a malfunctioning call may have its own errors on reproduction, creating a secondary cancer which stands to kill the original cancer. This may seem far-fetched but has a good grounding and is currently being further researched.
Genes – One of the more difficult to prove, although genes affect everything from how we look to our skin type. There is a very real possibility that there is just a certain nature of gene which suppresses cancer growth better than what we have.
Peto’s paradox is not the final answer, as there are outliers like the naked mole rate. A win is a win though just like at grandrush.com. In fighting cancer, any research opportunity is a good one, as any progress made stands to change millions of lives for the better.
La mémoire épisodique permet d’encoder, de stoker et de récupérer des souvenirs personnels en tenant compte du contexte spatial et temporel.
La mémoire épisodique peut être par exemple la capacité de se souvenir de ses vacances dans les Alpes l’hiver dernier.
C’est la principale forme de mémoire altérée dans le vieillissement dit pathologique, tel que par exemple la maladie d’Alzheimer.
Les personnes âgées en santé (c’est-à-dire qui ne présentent aucun trouble) ont également une moins bonne mémoire épisodique, par rapport à une personne plus jeune.
Une des raisons est que le sommeil en phase lente, bénéfique pour la consolidation de ce type de mémoire, est plus court chez la personne âgée
Une personne qui présente un déficit de mémoire épisodique a du mal à enregistrer une information, à la stocker et à la restituer.
effectue involontairement plusieurs fois le même achat dans la journée;
répète la même question;
ne sait plus qui elle vient de rencontrer;
ne se souvient plus de l’endroit où elle a garé sa voiture, rangé ses clés, son portefeuille etc;
finit par ne plus se souvenir de ce qu’elle a oublié.
Le cas du patient H.M.
Les connaissances sur le mémoire épisodique ont pris un grand essor avec la cas du patient Henry Molaison (1926-2008), connu sous les intiales H.M., grâce à qui il été permis de distinguer les origines de la mémoire dans le cerveau. Henry Molaison souffrait de graves crises d’épilepsie. En 1953, des chirurgiens ont prélevé une section de tissu de la taille d’un pouce de chaque côté de son cerveau. Les crises ont diminué, mais par la suite Molaison souffrait d’une amnésie permanente. Il pouvait se souvenir de certaines choses – des scènes de son enfance et des événements historiques survenus avant son opération – mais il était incapable de former de nouveaux souvenirs. S’il rencontrait quelqu’un qui quittait ensuite la pièce, en quelques minutes, il n’avait aucun souvenir de la personne.
La chercheuse Brenda Milner a étudié son cas et a montré que son lobe temporal (dont une partie avait été prélevée lors de la chirugie) ne lui permettait plus d’acquérir de nouveaux souvenirs, tout en préservant les souvenirs et autres fonctions cognitives qui étaient antérieurs à son opération.
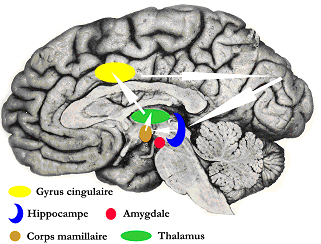
Un bon fonctionnement de la mémoire épisodique repose sur un bon fonctionnement de l’hippocampe, une structure du cerveau impliquée dans la mémoire et l’apprentissage. Ce dernier fait partie d’un réseau appelé circuit de Papez situé dans le système limbique.
Chez une personne âgée en bonne santé, il y un défaut d’encodage, c’est-à-dire un mauvaise mémorisation d’une nouvelle information captée par les organes des sens., du fait notamment d’une baisse de l’attention. Les stratégies de récupération de l’information sont également moins efficaces. Il n’existe en revanche peu de déficit de stockage de l’information.
Le médecin recense les antécédents médicaux et l’historique de la plainte du patient, et recherche des symptômes fréquemment rencontrés chez le patient âgé : perte nutritionnelle, apathie, troubles de la posture, douleurs, etc.
Il teste sa capacité à se situer dans le temps et l’espace.
Le patient peut alors effectuer un test (par exemple le Questionnaire de Mac Nair) qui lui permet d’apprécier la manière dont il perçoit la qualité de sa mémoire dans sa vie quotidienne.
Le médecin s’assure que ses capacités de jugement, déraisonnement, visuelles, spatiales sont intactes avant de lui faire passer un test plus spécifique d’évaluation de la mémoire épisodique.
Il existe des tests plus ou moins spécifiques d’évaluation de la mémoire qui sont:
Le trouble (ou état) de stress post-traumatique est un problème de santé mentale déclenché par un événement terrifiant, qu’il soit vécu ou témoin. Les symptômes peuvent inclure des cauchemars et un état d’anxiété sévère, ainsi que des pensées incontrôlables reliées à l’événement.
La plupart des personnes qui traversent des événements traumatisants peuvent avoir des difficultés temporaires à s’adapter et à faire face, mais avec du temps et de bons soins adaptées, elles s’améliorent généralement. Si les symptômes s’aggravent, durent des mois, voire des années, ils interfèrent avec le fonctionnement quotidien. La personne souffre lors de trouble d’état de stress post-traumatique.
Plus de 90 % des personnes souffrant d’un trouble mental sévère et persistant ont été exposées à un événement traumatique dans leur vie.
Les personnes agées ne sont pas plus à risque que les jeunes de développer un état de stress post-traumatique. Elles semblent même meux s’adapter. Les facteurs de stress rencontrées par les personnes âgées plus spécificquement sont :
Le deuil d’un proche
Le sens donnée aux expériences de la vie
La perte de sens
La perte de soutien social.
Dans la population général, les personnes plus à risque de souffrir d’un état de stress post-traumatique sont :
Les victimes de viol
Les militaires exposés au combat
Les victimes d’accidents de la route
Les intervenants de première ligne (policiers, pompiers et ambulanciers)
Critères diagnostiques de l’état de stress post-traumatique selon le manuel psychiatrique américain DSM-5
Le diagnostic de stress post-traumatique ne peut être posé qu’un mois après l’exposition à un événement traumatique (p. ex. viol, accident de voiture etc.).
Ces critères s’appliquent aux individus de plus 6 ans.
A. Exposition à la mort, à des blessures graves, ou à des violences sexuelles d’au moins une des façons suivantes :
Etre exposé directement l’événement traumatique.
Être témoin d’un ou plusieurs événements traumantique.
Apprendre que l’événement traumatique soit survenu à un membre de la famille proche ou un ami proche. Note : En cas de décès ou de danger de décès d’un membre de la famille ou d’un ami, l’événement doit avoir été violent ou accidentel.
Etre exposé de manière répétée ou extrême aux détails pénibles de l’événement traumatique. Note : Le critère A4 ne s’applique pas à l’exposition par le biais des médias électroniques, de la télévision ou d’images.
B. Présence d’un (ou plusieurs) des symptômes envahissants suivants associés à l’événement traumatique, ayant débuté après ce dernier :
Souvenirs pénibles récurrents, involontaires, et envahissants de l’événement traumatique, provoquant un sentiment de détresse.
Rêves répétitifs pénibles dans lesquels le contenu et/ou l’affect sont liés à l’événement traumatique.
Réactions dissociatives (p. ex. scènes rétrospectives) dans lesquelles le contenu est lié à l’événement traumatique.
Sentiment de détresse psychologique lors de l’exposition à des indices évoquant l’événement traumatique.
Réactions physiologiques marquées à des indices internes ou externes évoquant ou ressemblant à un aspect de l’événement traumatique.
C. Évitement persistant des stimuli associés à l’événement traumatique ayant débuté après sa survenue, comme en témoigne(nt) la présence d’une ou les deux manifestations suivantes :
Évitement ou efforts pour éviter les souvenirs, les pensées ou les sentiments pénibles liés à l’événement traumatique.
Évitement ou efforts pour éviter les rappels externes qui rappellent des souvenirs, des pensées ou des sentiments pénibles associés à l’événement traumatique.
D. Altérations négatives des cognitions et de l’humeur associées à l’événement traumatique, ayant débuté ou s’étant aggravées après ce dernier, comme en témoignent deux (ou plus) des manifestations suivantes :
Incapacité de se rappeler un aspect important de l’événement traumatique.
Croyances ou attentes négatives persistantes ou exagérées concernant soi-même, les autres, ou du monde (par exemple, « Je suis mauvais », « On ne peut faire confiance à personne »).
Distorsions cognitives persistantes concernant la cause ou les conséquences de l’événement traumatique qui amènent l’individu à se blâmer ou à blâmer d’autres personnes.
État émotionnel négatif persistant (par exemple, peur, horreur, colère, culpabilité ou honte).
Réduction marquée de l’intérêt ou de la participation à des activités importantes.
Sentiment de détachement ou de se sentir étranger vis-à-vis des autres.
Incapacité persistante de ressentir des émotions positives (par exemple, incapacité à éprouver du bonheur, de la satisfaction ou des sentiments affectueux).
E. Altérations marquées dans l’activation et la réactivité associées à l’événement traumatique, ayant débuté ou s’étant aggravées après ce dernier, comme en témoignent deux (ou plus) des manifestations suivantes :
Comportement irritable et accès de colère généralement sous forme d’agression verbale ou physique envers des personnes ou des objets.
Comportement irréfléchi ou autodestructeur.
Hypervigilance.
Réaction de sursaut exagérée.
Problèmes de concentration.
Troubles du sommeil (par exemple, difficultés à s’endormir ou sommeil agité).
F. La perturbation (critères B, C, D, et E) dure plus que 1 mois.
G. La perturbation entraîne une souffrance cliniquement significative ou une altération du fonctionnement au niveau social, professionnel ou autres domaines importants.
H. La perturbation n’est pas imputable aux effets physiologiques d’une substance (par exemple, médicaments, alcool) ou d’une autre maladie.
La mémoire de travail est la mémoire à capacité limitée qui permet de garder des information en mémoire quelques secondes. Par exemple, retenir par oral un numéro de téléphone avant de le composer ou se souvenir de l’objet que l’on doit aller récupérer lorsque l’on descend à la cave.
Elle travaille avec des « auxiliaires » qui permettent le stockage d’informations spatiales et verbale, la manipulation d’images mentales et la gestion des doubles tâches. Elle intervient dès lors qu’un contrôle et un partage de l’attention sont requis par les demandes de l’environnement.
Selon le modèle proposé par le scientifique Alan Baddeley (université de Cambridge), cette forme de mémoire comprend un système central de gestion des ressources de l’attention (administrateur central) et des sous-systèmes de maintien et de de traitement impliqué dans l’enregistrement de l’information verbale (boucle phonologique) et visuo-spatiale. C’est l’administrateur central qui est déficitaire dans la maladie d’Alzheimer.
Pour résumer:
Une boucle pholnologique qui maintient l’information verbale (p. ex j’enregistre verbalement un numéro de tétélphone)
Un système visuel et spatial qui a les même caractéristiques que la boucle phonologique mais qui est chargé d’enregistrer les informations visuelles et spatiales.
Un administrateur central qui est chargé de porter une attention à l’information.
L’arthrite est une maladie difficile à traiter qui fait souffrir des centaines de milliers de personnes dans le monde. Heureusement, des recherches avancées sur le cannabidiol ont démontré l’efficacité de la molécule du cannabis pour diminuer les symptômes de cette maladie inflammatoire. Il s’avère en effet que l’huile de CBD soit l’un des meilleurs traitements pour soulager l’arthrite. Comment s’en procurer et comment l’utiliser pour apaiser les douleurs de l’arthrite ? Eléments de réponses.
Weedy : un professionnel des produits CBD contre l’arthrite
Comme le CBD est un produit réglementé, il faut s’en procurer auprès d’un professionnel. Parmi les meilleurs fournisseurs du moment, il y a le spécialiste du CBD Weedy qui propose des produits de qualité. La boutique en ligne vous propose des produits à base de cannabidiol 100% légal. Ce qui veut dire que les taux de la molécule utilisée est inférieur à 0,2% pour l’ensemble de ses produits.
Sur le site, vous pouvez trouver toutes sortes d’articles que vous pouvez commander en toute discrétion. Aussi, vous avez la possibilité de suivre votre commande qui arrivera en moyenne dans les 24 à 72 heures suivant votre commande.
Tout une gamme de produit à base de CBD, dont l’huile de massage pour soulager l’arthrite vous est proposée. Appliquée sur les parties douloureuses, l’huile de CBD apaise les douleurs aigües. Il s’agit de la solution la plus intéressante du moment pour traiter cette pathologie. Bien que le CBD agit principalement sur les symptômes, non pas la maladie, il demeure toutefois d’une grande aide pour les souffrants de la maladie.
L’anti-inflammatoire naturel le plus efficace contre l’arthrite
Le plus souvent, ce sont les anti-inflammatoires non stéroïdiens qui sont utilisés pour calmer les symptômes. Toutefois, les inflammations provoquées par l’arthrite peuvent avoir des causes multiples et se manifester de plusieurs manières. En conséquence, les soins dépendent aussi en grande partie de ces facteurs.
Les corticoïdes font aussi partie des soins pour soulager les douleurs de l’arthrite. Seulement, ces traitements engendrent souvent des effets secondaires plus ou moins violents. En effet, les anti-inflammatoires chimiques peuvent affecter la digestion, affaiblir les muscles ou encore provoquer des complications oculaires. Ce qui constitue des risques conséquents pour les patients à risque.
En revanche, il n’y a pas d’effet secondaire avec le CBD, le cannabidiol présentant des particularités anti-douleur et anti-inflammatoire naturelles. Ainsi, l’huile de CBD ou les gels sont les meilleurs remèdes pour apaiser l’arthrite, en particulier l’arthrite chronique. En effet, la molécule de cannabis agit directement sur le système endocannabinoïde. Cela va aider le corps à profiter à nouveau de son homéostasie naturelle. Il stimule aussi les cellules anti-inflammatoires pour soulager les douleurs.
Le CBD pour traiter l’arthrose
Arthrose et arthrite peuvent prêter à confusion tant les pathologies sont similaires. Cependant, il y a bien une distinction entre l’arthrose, qui est une atteinte mécanique de l’articulation, et l’arthrite, qui est une atteinte inflammatoire. Mais la bonne nouvelle est que le CBD est aussi en mesure de traiter la douleur pour les deux maladies. En effet, le principe actif du CBD est aussi efficace pour traiter la douleur neuropathique articulaire de l’arthrose.
The neurotransmitter, often called a chemical messenger, is a molecule used by the nervous system to transmit messages between neurons or from neurons to muscles.
It is released at the end of neurons.
The neurotransmitter is one of the main protagonists of synaptic transmission.
More than fifty have been identified to date.
Communication between two neurons occurs in the synaptic cleft (the small space between the synapses of neurons).
The electrical signals that have traveled along the axon are converted into chemical signals by the release of neurotransmitters, eliciting a specific response in the downstream neuron, due to the neurotransmitter’s interaction with its receptor.
Neuromodulators are a bit different, as they are not limited to the synaptic gap between two neurons and therefore can affect a large number of neurons at once. Neuromotransmitters therefore regulate populations of neurons.
Most neurotransmitters are either small molecules of amines, amino acids, or neuropeptides.
To date, there are a dozen known small molecule neurotransmitters and over 100 different neuropeptides.
These chemicals and their interactions are involved in countless functions of the nervous system as well as in the control of bodily functions.
A neuron and its synaptic termination are identified by the neurotransmitter they produce and release: for example, a cholinergic neuron is a neuron that releases the acetylcholine neurotransmitter at its synapses.
Here are the main neurotransmitters, with their abbreviations and the corresponding qualifier in parentheses:
Neurotransmitter
Abbreviation
Qualifier
Acetylcholine
ACh
cholinergic
Dopamine
DA
dopaminergic
Noradrenaline
NA
noradrenergic
Serotonin
5-HT
serotonergic
Glutamate
Glu
glutamatergic
Gamma aminobutyric acid
GABA
gabarergic
A neurotransmitter influences a neuron in three ways: excitatory, inhibitory, or modulatory.
An excitatory neurotransmitter promotes the generation of an electrical signal called an action potential in the receptor neuron, while an inhibitory neurotransmitter prevents it. Whether a neurotransmitter is excitatory or inhibitory depends on the receptor to which it binds.
Examples of excitatory or inhibitory neurotransmitters
Neurotransmitter
Acetylcholine
Excitatory
Dopamine
Excitatory
Noradrenaline
Excitatory
Serotonin
Excitatory
Glutamate
Excitatory
GABA
Inhibitor
Neurotransmitters perform various functions in the brain when released; here are the main ones:
Neurotransmitter
Functions
Acetylcholine
Promotes attention, memory and learning Stimulates skeletal muscle contraction Dilation of the vessels Contraction of the bronchi, pupil, intestines Bradycardia (heart) Stimulates the excretion of certain hormones
Dopamine
Controls motor skills and psoture Coordinates certain cognitive and emotional processes Promotes attention Modulates mood Plays a role in addiction
Noradrenaline
Controls vigilance Promotes attention Adjusts certain behaviors such as stress, emotion Acts as a hormone in the blood by stimulating the contraction of blood vessels and increasing the heart rate.
Serotonin
Regulates mood Regulates the circadian cycle Pain control Regulates temperature Regulates appetite
Glutamate
Promotes long-term learning and memorization of information, plasticity of brain synapses
FRONT
Decreases the excitability of neurons It is mainly present in the neurons of the cortex. Contributes to motor control and vision.
An alteration in their function causes disturbances in the brain, causing disorders – cognitive, psychological and behavioral – depending on the neurotransmitter involved.
Here are some examples of neurotransmitters whose decrease or increase is associated with disorders or diseases.
Neurotransmitter
Alteration
Disorders and illnesses
Acetylcholine
Decrease
Alzheimer’s disease, Parkinson disease
Dopamine
Decrease
Parkinson disease
Dopamine
Increase
Schizophrenia and other psychotic disorders
Noradrenaline
Decrease
Alzheimer’s disease, Depression
Serotonin
Decrease
Depression
Glutamate
Increase
Stroke, Alzheimer’s disease
FRONT
Decrease
Epilepsy
What happens to neurotransmitters?
The neurotransmitters released by the vesicles will diffuse into the synaptic cleft in which:
They are degraded by enzymes , proteins that can be compared to scissors cutting in half a neurotransmitter to inactivate it.
They are re-captured by molecules (called transporters ) located on the membrane of the presynaptic neuron. These transporters ‘pump’ neurotransmitters for reuse. The neuron thus saves the synthesis of neurotransmitter. In general, the greater the release of neurotransmitter, the greater the activity of transporters.
They bind to proteins (called receptors ) located on the membrane of the presynaptic and postsynaptic neuron.
Receptors located on the membrane of the presynaptic neuron (called presynaptic receptors) control the release, synthesis and reuptake of the neurotransmitter.
The remaining amount of neurotransmitter (that is to say the amount that has not been degraded or recaptured) will bind to receptors located on the membrane of the postsynaptic neuron (we speak of postsynaptic receptor).
Binding of the neurotransmitter with its receptor will lead to a physiological effect (e.g. muscle contraction if the released neurotransmitter is acetylcholine
Where and how are they synthesized ?
They are synthesized by neurons in the nerve ending and / or the cell body. In the latter case, the chemical messenger migrates freely or is transported through the vesicles to the synaptic termination.
This synthesis is done from other molecules (called precursors) called substrates and involves (synthetic) enzymes which accelerate these reactions.
Here is a summary of the fate of a neurotransmitter:
When the nerve impulse arrives at the end of the neuron (1), the vesicles (2) release the neurotransmitters (3) into the synaptic cleft. These neurotransmitters will attach to receptors (4) located on the other neuron, inducing an electric current (5).
Le trouble de la personnalité limite (borderline) est un trouble de santé mentale qui affecte la façon dont on pense et dont on perçoit les autres. On a des difficultés à contenir ses émotions ou à maîtriser ses impulsions.
Le trouble de la personnalité limite est un trouble mental grave caractérisé par une incapacité à gérer efficacement ses émotions. Les relations sont affectées. Il débute généralement à l’adolescence ou au début de l’âge adulte. Image par Sascha Milk de Pixabay
Le trouble de la personnalité limite provoque des problèmes de
fonctionnement au quotidien. Cela comprend des problèmes d’image de soi,
des difficultés à gérer ses émotions et son comportement.
La personne a une peur intense de l’abandon ou de l’instabilité
et a du mal à tolérer la solitude.
Une colère inappropriée, une impulsivité et des sautes d’humeur
fréquentes peuvent éloigner les autres, même si la personne souhaite avoir des
relations aimantes et durables.
Le trouble de la personnalité limite commence généralement au
début de l’âge adulte. La maladie semble s’aggraver chez le jeune adulte
et peut s’améliorer progressivement avec l’âge.
De nombreuses personnes atteintes de ce trouble s’améliorent avec le temps et avec l’aide d’un traitement et peuvent apprendre à vivre une vie satisfaisante.
Historique
Le psychiatre Pinel décrit des personnes qui présentent des crises de colère et de violence, sans pour autant être aliénées. Par la suite, d’autres psychiatres ont décrit différents types de personnalité : shizoide, cyclothymique, asthénique et autistique.
C’est à partir des années 30 que le concept de trouble de la personnalité entre la névrose et la psychose a été élaborée. Ce terme a été utilisé pour la première fois par Stern en 1938.
Les deux premiers manuels de psychiatrie proposent des types de personnalités : paranoide, schizoide, cyclothymique et sociopathique.
Epidémiologie
La prévalence des différentes formes de personnalité limite se situe entre 0,5% (personnalité narcissique) et 2% (personnalité obsessionnelle-compulsive). Les autres prévalences se situent entre ces pourcentages (schizoide, schizotypique, histrionique, antisociale, narcissique, .vitante, dépendante).
La présence d’autres troubles psychiatriques est très courant.
Les personnalités bizarres et excentriques présentent des troubles psychotiques, mais aussi des trobules de comportements perturbateurs et anxieux.
Les personnalités intenses et dramatiques présentent des troubles de l’humeur et de contrôle des impulsions.
Les personnalités anxieuses présentent des troubles anxieux et dépressifs.
Symptômes de la personnalité borderline
Le trouble de la personnalité limite affecte ce que vous
ressentez pour vous-même, vos relations avec les autres et votre comportement.
Les signes et symptômes peuvent inclure:
Une peur intense de l’abandon, allant même jusqu’à des
comportements extrêmes pour éviter une séparation ou un rejet réel ou
imaginaire.
Un modèle de relations intenses instables, comme l’idéalisation
de quelqu’un à un moment, puis le fait de croire soudainement que la personne
n’est pas la bonne personne.
Changements rapides de l’identité de soi et de l’image de soi.
Périodes de paranoïa liée au stress et de perte de contact avec
la réalité, d’une durée de quelques minutes à quelques heures.
Comportement impulsif et risqué, comme le jeu, la conduite
imprudente, les rapports sexuels non protégés, les dépenses inconsidérées, la
consommation de drogues ou le désire de briser un bon parcours (par ex. quitter soudainement un bon emploi).
Menaces ou comportements suicidaires ou automutilation, souvent
en réponse à la peur de la séparation ou du rejet.
De larges sautes d’humeur d’une durée de quelques heures à
quelques jours.
Sentiments continus de vide
Colère inappropriée et intense, telle que perdre fréquemment son
sang-froid, être sarcastique ou amer ou avoir des bagarres physiques
Causes du trouble de la personnalité limite
Comme pour les autres troubles de santé mentale, les causes du trouble de la personnalité limite ne sont pas entièrement compris. En plus des facteurs environnementaux – tels que des antécédents de maltraitance ou de négligence envers les enfants – le trouble de la personnalité limite peut être lié à :
La génétique.
Anomalies cérébrales. Certaines recherches ont montré des changements dans certaines zones du cerveau impliquées dans la régulation des émotions, l’impulsivité et l’agression.
Certains médecins ont émis l’hypohtèse que des triats de personnalité présents dès l’enfance peuvent être des facteurs de risque : comportement agressif dès la maternelle, phobie sociale.
Les études de neuroimagerie ont rapporté chez certains patients une augmentation de la taille des ventricules cérébraux et une légère atrophie du lobe frontal. Cependant, l’activité du lobe frontal est préservée.
Ches les adultes souffrant de trouble de personnalité limite, il a été également rapporté que les volumes de certaines structures du système limbique – amygdale, hippocampe – sont diminuées. L’activité de l’amygdale serait plus importante chez ces personnes lorsqu’on leur présente des images émotionnellement chargées.
Selon certaines psychologues, le trouble de la personnalité serait l’expression extrême de traits de personnalité que l’on observe dans la population en général. Ces traits de personnalité ont notammenet été décrits par McCrae $ Costa avec le modèle Big Five (1990).
Ouverture à l’expérience : appréciation des idées nouvelles, originales, de l’aventure…
Caractère consciencieux: fiabilité, ordonné, rigoureu, respecteux des normes…
Extraversion : jovial, fonceur, facilité à s’exprimer…
Névrotisme : tendance à la détresse, l’anxiété, à la tristesse et/à la colère
Les individus avec une trouble de personnalité limite on un niveau élevé de névrotisme.
Facteurs de risque
Certains facteurs liés au développement de la personnalité
peuvent augmenter le risque de développer un trouble de la personnalité
limite. Ceux-ci inclus:
Prédisposition héréditaire. Vous courez peut-être un risque plus élevé si un parent proche – votre mère, votre père, votre frère ou votre sœur – a le même trouble ou un trouble similaire.
Une enfance stressante. De nombreuses personnes atteintes de ce trouble déclarent avoir été victimes de violence sexuelle ou physique.
Il existe d’autres facteurs qui, hormis les expériences d’abus, augmentent le risque de trouble de personnalité limite:
Faible niveau socio-économique.
Mauvaise entente entre parents.
Conduites antisociales des parents.
Maladie ou décès d’un ou des deux parents en bas âge.
Facteurs associés à un manque d’attachement parent-enfant : punitions trop sévères, grossesse non désirée, faible proximité physique ou psychologique avec la mère ou le père.
Complications
Le trouble de la personnalité limite peut endommager de nombreux
domaines de la vie. Cela peut affecter négativement les relations intimes,
l’emploi, l’école, les activités sociales et l’image de soi, entraînant:
Changements ou pertes d’emploi répétés.
Études non achevées.
Problèmes avec la justice, tels qu’une peine de prison.
Relations conflictuelles, stress conjugal ou divorce.
Automutilation (coupure ou brûlure) et hospitalisations
fréquentes.
Implication dans des relations abusives.
Grossesses non planifiées, infections sexuellement transmissibles,
accidents de la route et bagarres dues à des comportements impulsifs et à
risque.
Tentative de suicide ou suicide.
De plus, ce trouble s’accompagne d’autres troubles de santé
mentale, tels que:
Un diagnostic de trouble de la personnalité limite est généralement posé chez les adultes et non chez les enfants ou les adolescents. En effet, ce qui semble être des signes et des symptômes de trouble de la personnalité limite peut disparaître à mesure que les enfants deviennent plus matures.
Les critères diagnostiques sont établis selon le modèle de classification du manuel DSM-5 qui est le suivant :
Tous les individus présentent les traits (différents de troubles) de personnalité suivants (identité, autodétermination, empathie, intimité) qui sont associés à différents domaines et à des niveaux différents :
Niveau 0 : peu ou pas d’altération
Niveau 1 : un certain niveau d’altération
Niveau 2 : altération moyenne
Niveau 3 : altération grave
Niveau 4 : altération extrême
Domaine 1 : Affectivité négative
Expériences fréquentes et intenses d’une large gamme d’émotions négatives
Labilité émotionnelle
Tendance anxieuse
Insécurité liée à la séparation
Tendance à la soumission
Hostilité
Persévération
Dépressivité
Méfiance
Affectivité restreinte
Domaine 2 : détachement
Retrait des interactions interpersonnelles et restriction de l’expérience et de l’expression affectives.
Retrait
Evitement de l’intimité
Anhédonie
Dépressivité
Affectivité restreinte
Méfiance
Domaine 3 : antagonisme
Comportements qui mettent l’individu en désaccord avec autrui, avec un sens exagéré de sa propre importance.
Tendances manipulatoires
Malhonnêteté
Sentiment de grandeur, de supériorité, que tout lui est dû
Recherche d’attention
Dureté, insensibilité
Domaine 4 : désinhibition
Irresponsabilité : ne suit pas ses engagements, ne respecte pas ses promesses…
Impulsivité : agit sur un coup de tête, difficulté à élaborer et à suivre des plans…
Distractibilité : difficulté à se concentrer…
Prise de risque : s’engage dans des activités dangereuses, poursuite imprudente d’objectifs…
Traitement
Le trouble de la personnalité limite est principalement traité
par psychothérapie, mais des médicaments peuvent être prescrits.
Le médecin peut également recommander une hospitalisation si la
sécurité du patient est menacée.
Le traitement peut aider à faire face à la maladie. Il est
également nécessaire de se faire soigner pour tout autre trouble de santé
mentale qui survient souvent avec un trouble de la personnalité limite, tel que
la dépression ou la toxicomanie.
Psychothérapie
La psychothérapie – également appelée thérapie par la parole –
est une approche de traitement fondamentale pour le trouble de la personnalité
limite. Les objectifs de la psychothérapie sont :
De se concentrer sur sa capacité actuelle à fonctionner
D’apprendre à gérer ses émotions
Réduire l’impulsivité en observant ses sentiments plutôt qu’en
agissant sur eux
Travailler à améliorer ses relations en étant conscient de ses
sentiments et de ceux des autres
Les types de psychothérapie qui se sont révélés efficaces incluent:
Thérapie comportementale dialectique. Proposée par Linehan , cette thérapie a montré son efficacité chez les personnes avec des difficultés relationnelles, puis dans les troubles mentaux liés aux substances ou les troubles alimentaires. C’est une approche qui propose des interventions visant à apporter des changements (résolution de problèmes) et à accepter ses troubles. La période de traitement est d’au moins un an.
Thérapie centrée sur le schéma.
Thérapie basée sur la mentalisation quimet l’accent sur la réflexion avant de réagir.
Médicaments
Certains médicaments peuvent aider à soulager les symptômes ou
les problèmes concomitants tels que la dépression, l’impulsivité, l’agressivité
ou l’anxiété. Les médicaments incluent des antidépresseurs, des
antipsychotiques ou des médicaments stabilisateurs de l’humeur.
Hospitalisation
Parfois, il est nécessaire d’avoir besoin d’un traitement plus
intense dans un hôpital ou une clinique psychiatrique. L’hospitalisation
peut également protéger le patient de l’automutilation ou des comportements
suicidaires.
Rétablissement
Apprendre à gérer ses émotions, ses pensées et ses comportements
prend du temps. La plupart des gens s’améliorent considérablement, mais
ils peuvent toujours lutter contre certains symptômes du trouble de la personnalité
limite.
Les chances de succès augmentent lorsque le patient consulte un
professionnel de la santé mentale qui a de l’expérience dans le traitement du
trouble de la personnalité limite.
Commentaires fermés sur Mémoire déclarative (ou explicite)
La mémoire déclarative (ou mémoire explicite) est une mémoire qui a trait aux connaissances du monde qui nous entoure.
Elle n’apparaît pas à la naissance contrairement à la mémoire implicite mais plutôt après l’âge de 2 ans.
C’est une des deux formes de mémoire à long terme avec la mémoire implicite (ou non déclarative).
La mémoire explicite permet de retrouver des souvenirs de type sémantique, factuelles (p. ex. se rappeler d’un fait précis, qu’ils soient courants ou historiques) ou autobiographiques (se rappeler les événements de notre vie personnelle).
L’hippocampe, une structure du cerveau faisant partie du système limbique, est impliquée dans l’encodage de l’information, alors que le cortex cérébral intervient dans la consolidation de la mémoire à long terme.
Elle joue un rôle important dans l’apprentissage d’habiletés et d’habitudes acquises à partir de pratiques répétitives ; elle s’exprime sous forme d’actions automatisées (ex. faire du vélo, conduire une voiture, lacer ses chaussures, etc.) : c’est le système mnésique du « savoir-faire ».
La mémoire implicite est liée à des apprentissages perceptuels, émotionnels et comportementaux.
Les structures du cerveau impliquées dans la mémoire implicite sont situées dans le système limbique, soit :
L’amygdale pour la mémoire émotionnelle.
Les noyaux gris centraux (ou ganglions de la base) et le cortex moteur pour la mémoire motrice.
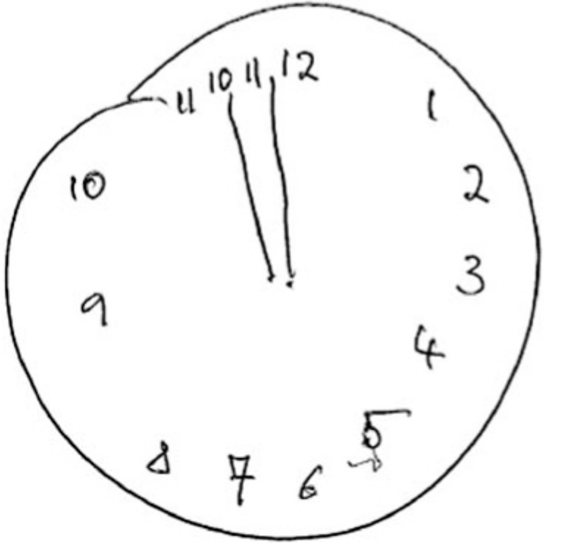
The clock drawing test is a quick and easy test to use to screen for impairments in cognitive functions such as praxis , attention, language, orientation in time and space, and executive functions.
Despite its simplicity, it is very sensitive, that is to say it can reliably detect this type of disorder.
What does the clock test consist of?
The examiner presents the subject with a sheet on which a circle of about 10 cm is drawn (the examiner can also ask the subject to draw the dial himself). Then he said to her:
“This circle represents the face of a clock (or a watch). Please place numbers in this circle so that it looks like a clock face. Then draw me hands showing the time of 11:10 ”(this time is particularly useful for subtly detecting a cognitive deficit, in particular a visual field disorder).
How to interpret the results?
The examiner checks the following four criteria:
The location of the numbers corresponding to each hour.
Scheduling of hours.
The correct representation of the two needles (small and large).
The location of the two hands corresponding to the requested time.
If the subject passes the clock test, the likelihood of having dementia is very low.
However, one or more errors indicate the presence of cognitive impairment or dementia . An additional test (in this case the MMSE test ) is necessary to undertake a more detailed assessment of cognitive functions.
Here is an example of drawing made by elderly subjects with dementai for example during the clock drawing test.
Example of a person with a cognitive deficit who did not pass the clock test. The hands and numbers are incorrectly positioned.